

Zanubrutinib Versus Ibrutinib in Symptomatic Waldenström Macroglobulinemia: Final Analysis From the Randomized Phase III ASPEN Study
- PMID: 37478390
- PMCID: PMC10666987
- DOI: 10.1200/JCO.22.02830
Zanubrutinib Versus Ibrutinib in Symptomatic Waldenström Macroglobulinemia: Final Analysis From the Randomized Phase III ASPEN Study
Abstract
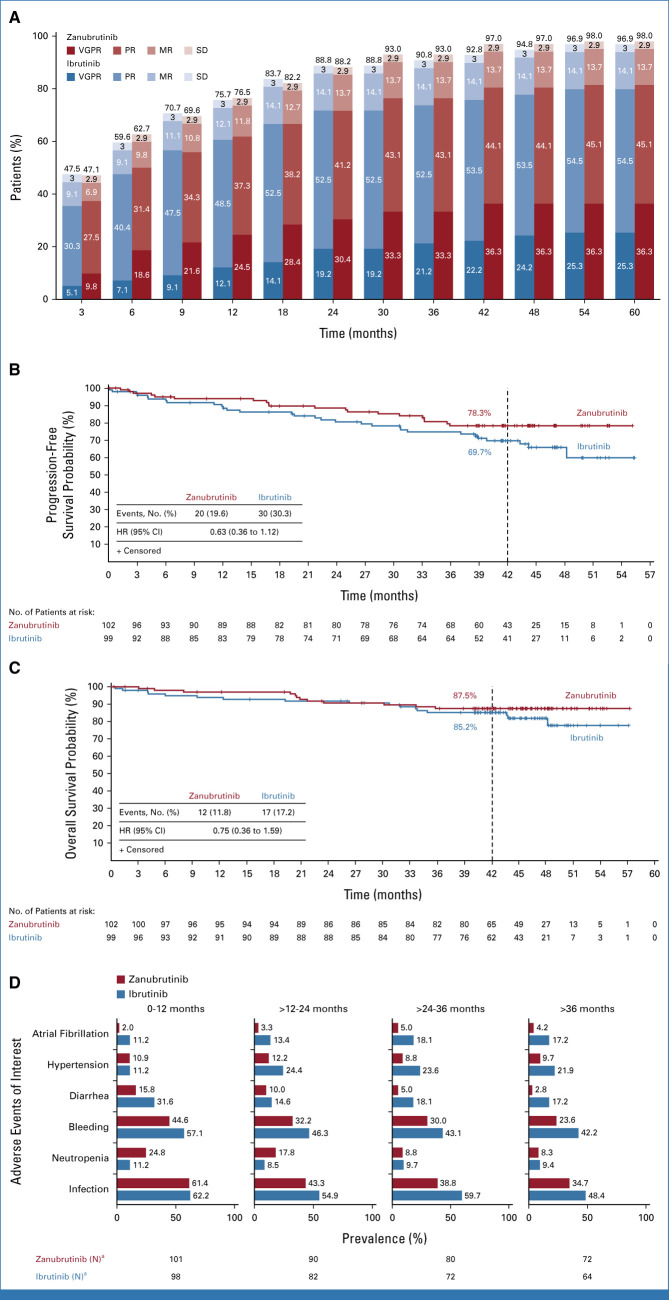
The phase III ASPEN study demonstrated the comparable efficacy and improved safety of zanubrutinib versus ibrutinib in patients with Waldenström macroglobulinemia (WM). Here, we report long-term follow-up outcomes from ASPEN. The primary end point was the sum of very good partial response (VGPR) + complete response (CR) rates; secondary and exploratory end points were also reported. Cohort 1 comprised 201 patients (myeloid differentiation primary response 88-mutant WM: 102 receiving zanubrutinib; 99 receiving ibrutinib); cohort 2 comprised 28 patients (myeloid differentiation primary response 88 wild-type WM: 28 zanubrutinib; 26 efficacy evaluable). At 44.4-month median follow-up, VGPR + CR rates were 36.3% with zanubrutinib versus 25.3% with ibrutinib in cohort 1 and 30.8% with one CR in cohort 2. In patients with CXC motif chemokine receptor 4 mutation, VGPR + CR rates were 21.2% with zanubrutinib versus 10.0% with ibrutinib (cohort 1). Median progression-free survival and overall survival were not reached. Any-grade adverse events (AEs) of diarrhea (34.7% v 22.8%), muscle spasms (28.6% v 11.9%), hypertension (25.5% v 14.9%), atrial fibrillation/flutter (23.5% v 7.9%), and pneumonia (18.4% v 5.0%) were more common with ibrutinib versus zanubrutinib; neutropenia (20.4% v 34.7%) was less common with ibrutinib versus zanubrutinib (cohort 1). Zanubrutinib was associated with lower risk of AE-related treatment discontinuation. Overall, these findings confirm the long-term response quality and tolerability associated with zanubrutinib.
Trial registration: ClinicalTrials.gov NCT03053440.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
References
-
- Guo Y, Liu Y, Hu N, et al. : Discovery of zanubrutinib (BGB-3111), a novel, potent, and selective covalent inhibitor of Bruton's tyrosine kinase. J Med Chem 62:7923-7940, 2019 - PubMed
-
- BRUKINSA [package insert]. San Mateo, CA. BeiGene USA, Inc, 2021
-
- BRUKINSA [product monograph]. BeiGene Switzerland GmbH. 2021
-
- National Medical Products Administration: Approved drug data search. https://www.nmpa.gov.cn/datasearch/
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
