

Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial
- PMID: 37478886
- PMCID: PMC10529382
- DOI: 10.1016/S0140-6736(23)01406-X
Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial
Abstract
Background: Hearing loss is associated with increased cognitive decline and incident dementia in older adults. We aimed to investigate whether a hearing intervention could reduce cognitive decline in cognitively healthy older adults with hearing loss.
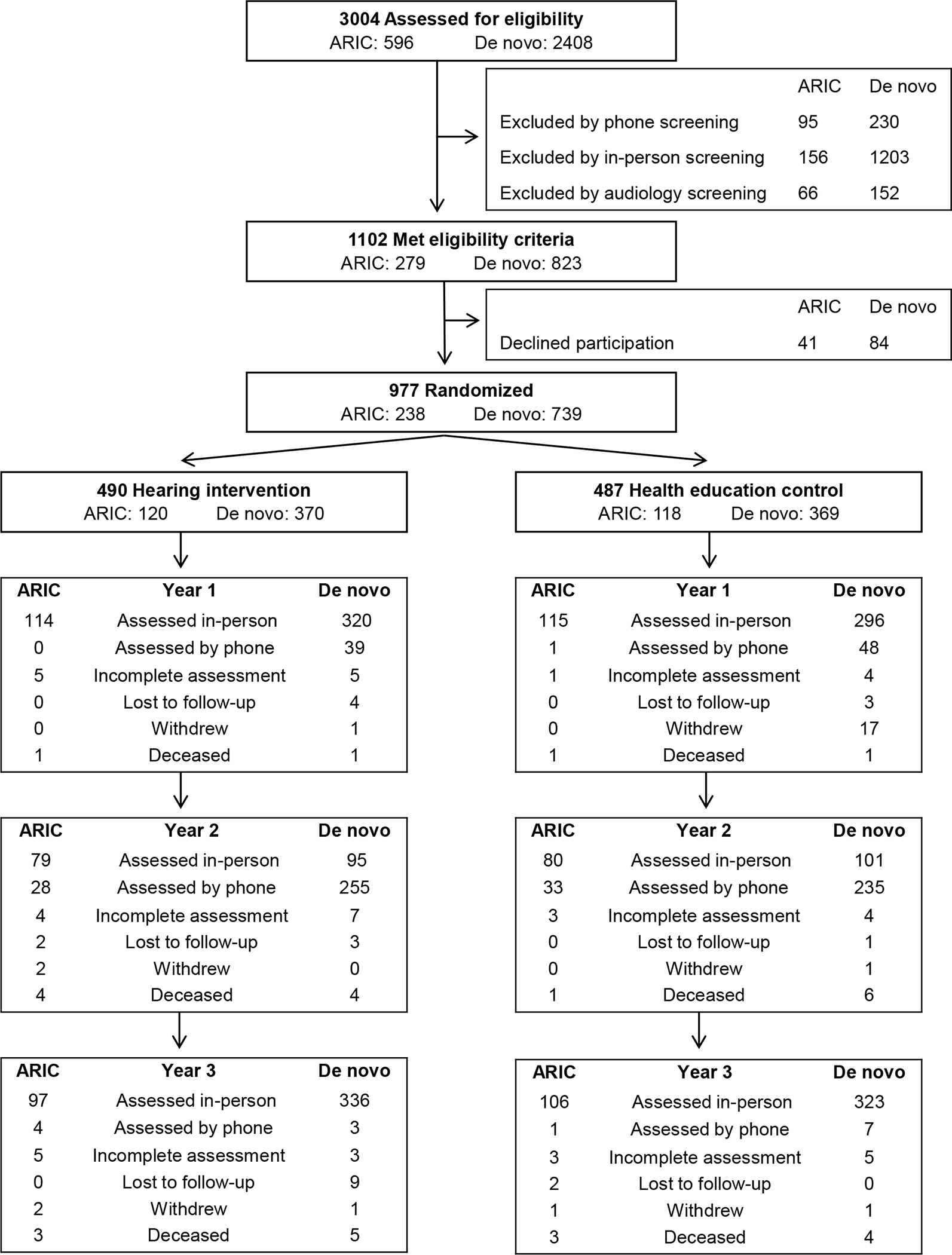
Methods: The ACHIEVE study is a multicentre, parallel-group, unmasked, randomised controlled trial of adults aged 70-84 years with untreated hearing loss and without substantial cognitive impairment that took place at four community study sites across the USA. Participants were recruited from two study populations at each site: (1) older adults participating in a long-standing observational study of cardiovascular health (Atherosclerosis Risk in Communities [ARIC] study), and (2) healthy de novo community volunteers. Participants were randomly assigned (1:1) to a hearing intervention (audiological counselling and provision of hearing aids) or a control intervention of health education (individual sessions with a health educator covering topics on chronic disease prevention) and followed up every 6 months. The primary endpoint was 3-year change in a global cognition standardised factor score from a comprehensive neurocognitive battery. Analysis was by intention to treat. This trial was registered at ClinicalTrials.gov, NCT03243422.
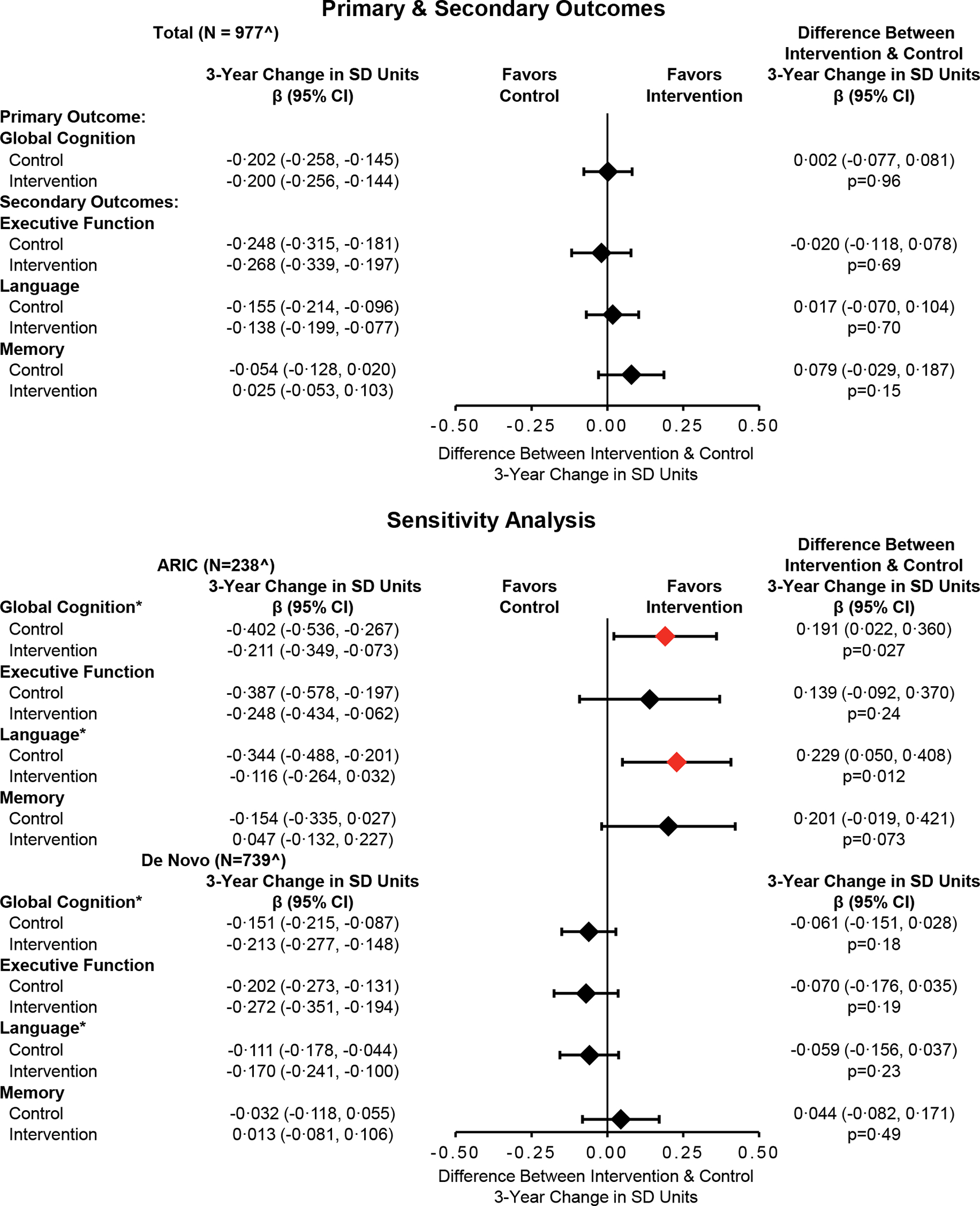
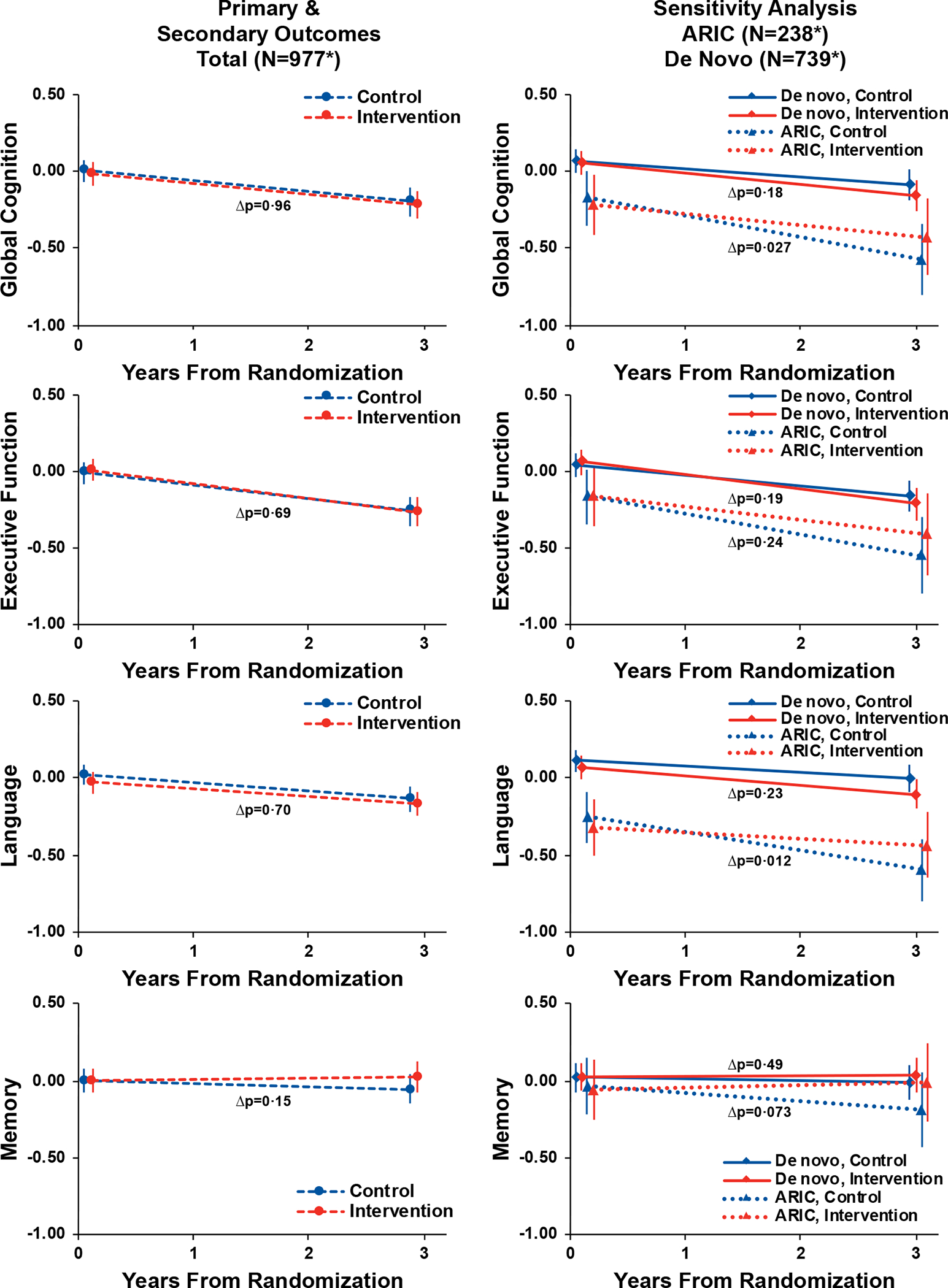
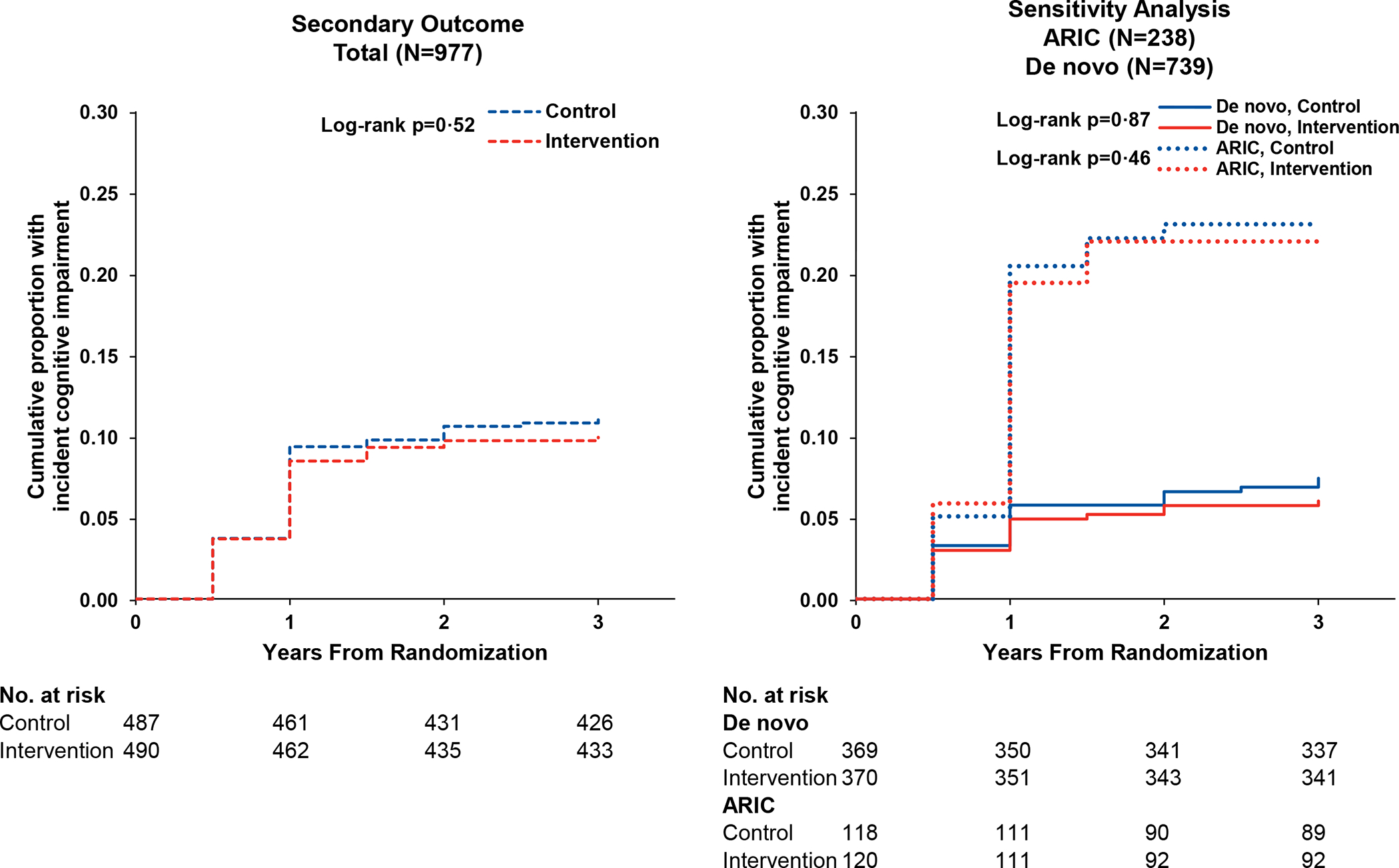
Findings: From Nov 9, 2017, to Oct 25, 2019, we screened 3004 participants for eligibility and randomly assigned 977 (32·5%; 238 [24%] from ARIC and 739 [76%] de novo). We randomly assigned 490 (50%) to the hearing intervention and 487 (50%) to the health education control. The cohort had a mean age of 76·8 years (SD 4·0), 523 (54%) were female, 454 (46%) were male, and most were White (n=858 [88%]). Participants from ARIC were older, had more risk factors for cognitive decline, and had lower baseline cognitive scores than those in the de novo cohort. In the primary analysis combining the ARIC and de novo cohorts, 3-year cognitive change (in SD units) was not significantly different between the hearing intervention and health education control groups (-0·200 [95% CI -0·256 to -0·144] in the hearing intervention group and -0·202 [-0·258 to -0·145] in the control group; difference 0·002 [-0·077 to 0·081]; p=0·96). However, a prespecified sensitivity analysis showed a significant difference in the effect of the hearing intervention on 3-year cognitive change between the ARIC and de novo cohorts (pinteraction=0·010). Other prespecified sensitivity analyses that varied analytical parameters used in the total cohort did not change the observed results. No significant adverse events attributed to the study were reported with either the hearing intervention or health education control.
Interpretation: The hearing intervention did not reduce 3-year cognitive decline in the primary analysis of the total cohort. However, a prespecified sensitivity analysis showed that the effect differed between the two study populations that comprised the cohort. These findings suggest that a hearing intervention might reduce cognitive change over 3 years in populations of older adults at increased risk for cognitive decline but not in populations at decreased risk for cognitive decline.
Funding: US National Institutes of Health.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests FRL reports research grants from the US National Institutes of Health and Eleanor Schwartz Charitable Foundation; consulting fees from Frequency Therapeutics and Apple; payment for expert testimony and participation on a scientific advisory board for Fondation Pour L'Audition and Sharper Sense; being a volunteer board member for Access HEARS; donation in-kind from Sonova/Phonak to Johns Hopkins University for hearing technologies used in the present study; and being the director of a public health research centre funded in part by a philanthropic donation from Cochlear to the Johns Hopkins Bloomberg School of Public Health. KMH reports consulting fees from Fred Hutchinson Cancer Research Center; support for attending meetings (National Institute for Health Center for Scientific Review and Hebrew Senior Life); participation on the Wake Forest School of Medicine DSMB (unpaid); and leadership roles for peer-reviewed journals (Alzheimer's & Dementia: Translational Research and Clinical Interventions and Alzheimer's & Dementia: Diagnosis, and Assessment & Disease Monitoring [unpaid]). DK serves on a DSMB for the Dominantly Inherited Alzheimer Network Treatment Unit study. He served on a DSMB for a tau therapeutic for Biogen (until 2021) but received no personal compensation. He is an investigator in clinical trials sponsored by Biogen, Lilly Pharmaceuticals, and the University of Southern California. He has served as a consultant for Roche, Samus Therapeutics, Magellan Health, Biovie, and Alzeca Biosciences but receives no personal compensation. He attended an Eisai advisory board meeting for lecanemab on Dec 2, 2022, but received no compensation. VS reports industry-sponsored clinical research contract (to institution) to support research activity from Otonomy, Frequency Therapeutics, Pipeline Therapeutics, Aerin Medical, Oticon Medical, and Helen of Troy; consulting fees from Autifony Therapeutics and Boehringer Ingelheim; honoraria from Oticon Medical, Sonova Holding, and Phonak USA; and hearing technology devices donated for educational or research proposes from Sonova Holding and Phonak USA. MA reports consulting fees from GN Resound, National Institute on Deafness and Other Communication Disorder (NIDCD), and the National Institute on Aging (NIA); travel support from NIDCD and NIA; and receipt of equipment from Sonova. NSR reports being Editor of the American Journal of Audiology (paid) and Scientific Chair of the American Academy of Audiology, Advisory Board Member with stock options for Neosensory, and being a member of the Scientific Advisory Board for Shoebox. All other authors declare no competing interests.
Figures
Comment in
-
Interventions to prevent dementia should target those at high risk.Lancet. 2023 Sep 2;402(10404):750-751. doi: 10.1016/S0140-6736(23)01472-1. Epub 2023 Jul 18. Lancet. 2023. PMID: 37478885 No abstract available.
-
Hörgerät reduziert kognitiven Abbau bei Demenzrisiko.MMW Fortschr Med. 2024 May;166(8):24-26. doi: 10.1007/s15006-024-3880-9. MMW Fortschr Med. 2024. PMID: 38693374 German. No abstract available.
-
Hearing intervention and cognitive decline: the ACHIEVE trial.Lancet. 2024 Jul 6;404(10447):29. doi: 10.1016/S0140-6736(24)00711-6. Lancet. 2024. PMID: 38971589 No abstract available.
-
Hearing intervention and cognitive decline: the ACHIEVE trial.Lancet. 2024 Jul 6;404(10447):29-30. doi: 10.1016/S0140-6736(24)00712-8. Lancet. 2024. PMID: 38971590 No abstract available.
References
-
- Alzheimer’s Disease International. Numbers of people with dementia around the world. https://www.alzint.org/resource/numbers-of-people-with-dementia-worldwide. Accessed May 8, 2023.
-
- World Health Organization. Risk reduction of cognitive decline and dementia : WHO guidelines. World Health Organization,; 2019:1 online resource (1 PDF file (xiv, 78 pages)). https://www.ncbi.nlm.nih.gov/books/NBK542796/ NLM Bookshelf Books - PubMed
-
- Mukadam N, Sommerlad A, Huntley J, Livingston G. Population attributable fractions for risk factors for dementia in low-income and middle-income countries: an analysis using cross-sectional survey data. Lancet Glob Health. May 2019;7(5):e596–e603. doi: 10.1016/S2214-109X(19)30074-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01 AG055426/AG/NIA NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- R01 AG060502/AG/NIA NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- R34 AG046548/AG/NIA NIH HHS/United States
- T32 AG000181/AG/NIA NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
