

Testing the causal relationships of physical activity and sedentary behaviour with mental health and substance use disorders: a Mendelian randomisation study
- PMID: 37479783
- PMCID: PMC10618087
- DOI: 10.1038/s41380-023-02133-9
Testing the causal relationships of physical activity and sedentary behaviour with mental health and substance use disorders: a Mendelian randomisation study
Abstract
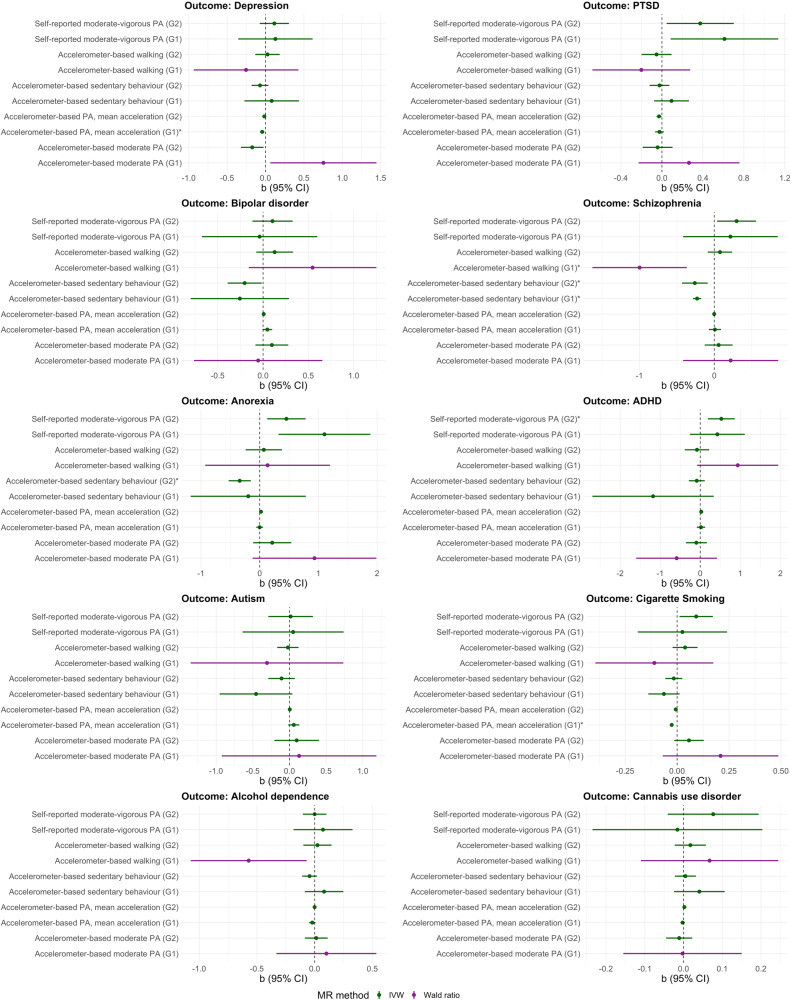
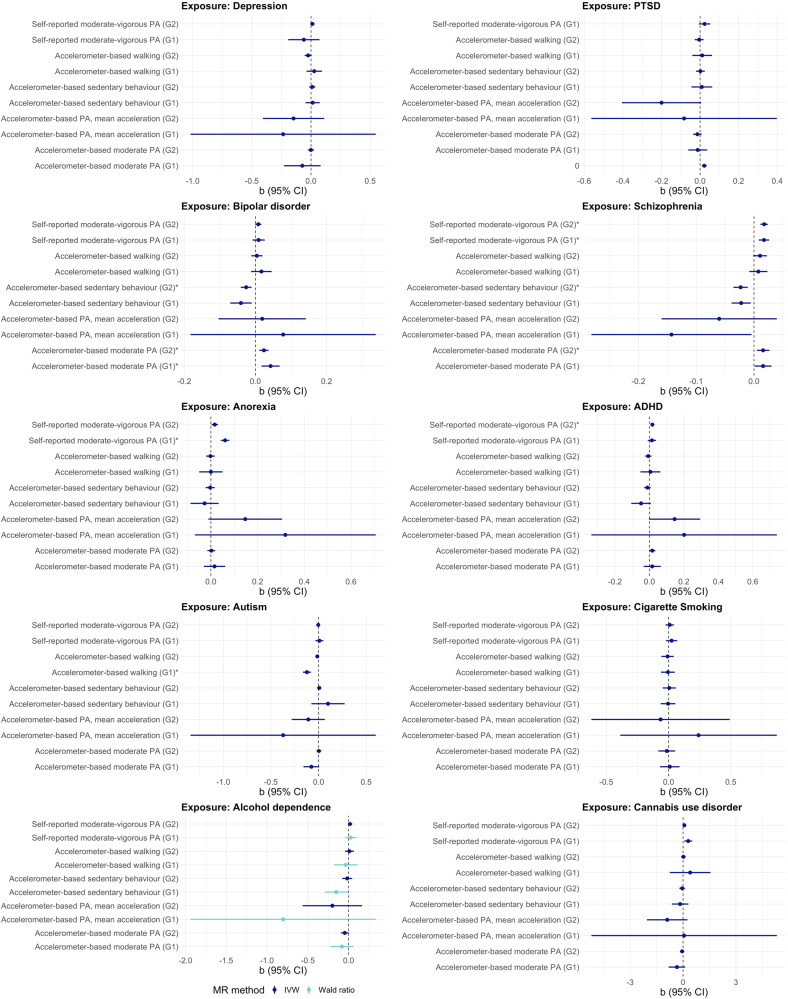
Observational studies suggest that physical activity can reduce the risk of mental health and substance use disorders. However, it is unclear whether this relationship is causal or explained by confounding bias (e.g., common underlying causes or reverse causality). We investigated the bidirectional causal relationship of physical activity (PA) and sedentary behaviour (SB) with ten mental health and substance use disorders, applying two-sample Mendelian Randomisation (MR). Genetic instruments for the exposures and outcomes were derived from the largest available, non-overlapping genome-wide association studies (GWAS). Summary-level data for objectively assessed PA (accelerometer-based average activity, moderate activity, and walking) and SB and self-reported moderate-to-vigorous PA were obtained from the UK Biobank. Data for mental health/substance use disorders were obtained from the Psychiatric Genomics Consortium and the GWAS and Sequencing Consortium of Alcohol and Nicotine Use. MR estimates were combined using inverse variance weighted meta-analysis (IVW). Sensitivity analyses were conducted to assess the robustness of the results. Accelerometer-based average PA was associated with a lower risk of depression (b = -0.043, 95% CI: -0.071 to -0.016, effect size[OR] = 0.957) and cigarette smoking (b = -0.026; 95% CI: -0.035 to -0.017, effect size[β] = -0.022). Accelerometer-based SB decreased the risk of anorexia (b = -0.341, 95% CI: -0.530 to -0.152, effect size[OR] = 0.711) and schizophrenia (b = -0.230; 95% CI: -0.285 to -0.175, effect size[OR] = 0.795). However, we found evidence of reverse causality in the relationship between SB and schizophrenia. Further, PTSD, bipolar disorder, anorexia, and ADHD were all associated with increased PA. This study provides evidence consistent with a causal protective effect of objectively assessed but not self-reported PA on reduced depression and cigarette smoking. Objectively assessed SB had a protective relationship with anorexia. Enhancing PA may be an effective intervention strategy to reduce depressive symptoms and addictive behaviours, while promoting sedentary or light physical activities may help to reduce the risk of anorexia in at-risk individuals.
© 2023. The Author(s).
Conflict of interest statement
BS is on the Editorial Board of Ageing Research Reviews, Mental Health and Physical Activity, The Journal of Evidence Based Medicine, and The Brazilian Journal of Psychiatry. BS has received honorarium from a co-edited book on exercise and mental illness and advisory work from ASICS Europe BV for unrelated work.
Figures

References
-
- Degenhardt L, Charlson F, Ferrari A, Santomauro D, Erskine H, Mantilla-Herrara A, et al. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. 2018;5:987–1012. - PMC - PubMed
