

Prevalence of dyslipidemia and its associated factors among university academic staff and students in Bangladesh
- PMID: 37479968
- PMCID: PMC10362587
- DOI: 10.1186/s12872-023-03399-1
Prevalence of dyslipidemia and its associated factors among university academic staff and students in Bangladesh
Abstract
Background: Dyslipidemia is one of the important contributors to cardiovascular disease and type 2 diabetes. There is little or no information on dyslipidemia among academic staff and students in Bangladesh. Therefore, this study aimed to investigate the prevalence and factors related to dyslipidemia among university academic staff and students in Bangladesh.
Methods: A total of 533 participants (302 academic staff and 231 students) were enrolled in this cross-sectional study. A simple random sampling technique was used to enrol the participants. Fasting blood samples were obtained from the participants, and serum levels of triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) were measured using the standard methods. Dyslipidemia was defined according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP-III) model guideline. Multivariable logistic regression was conducted to identify the factors related to lipid marker abnormalities.
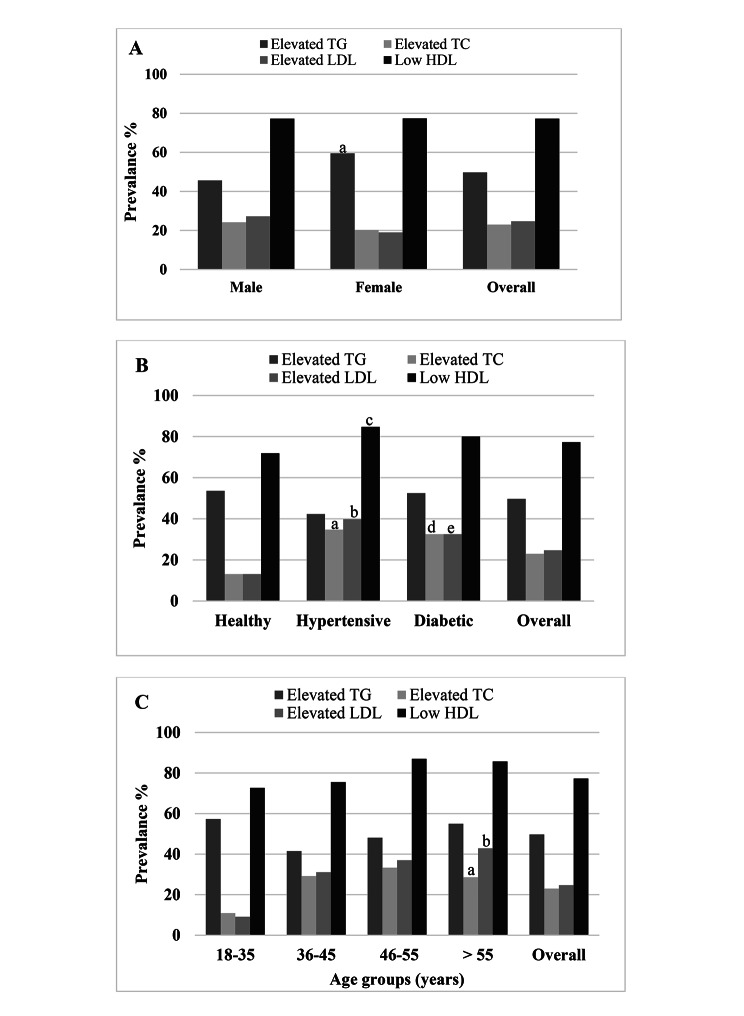
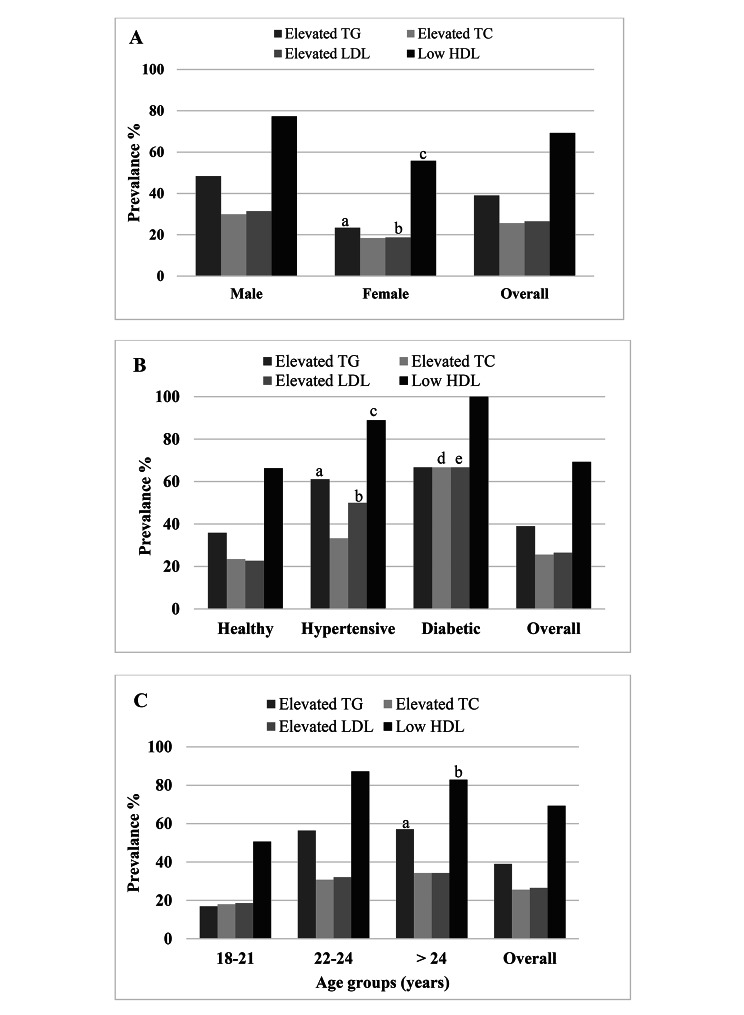
Results: Overall, the prevalence of dyslipidemia was 81.5%, of which 85% was in staff and 76.5% in students. A significant difference was found in the prevalence of dyslipidemia between males and females only in the student group (p < 0.01). Among staff, hypertriglyceridemia prevalence was 49.7%, hypercholesterolemia 23%, high LDL-C 24.7% and low HDL-C 77.3%. On the other hand, hypertriglyceridemia prevalence was 39%, hypercholesterolemia 25.6%, high LDL-C 26.5% and low HDL-C 69.3% among students. The most common lipid abnormality was low HDL-C in both groups. The prevalence of mixed dyslipidemia was 14.2% and 14.1% in staff and students, respectively. According to the regression analysis, increased age, obesity, diabetes, and inadequate physical activity were significantly associated with dyslipidemia.
Conclusions: Dyslipidemia was prevalent among the majority of the study participants. Increased age, obesity, diabetes, and inadequate physical activity were significantly associated with dyslipidemia. The study's results highlight the importance of implementing interventions to address the associated risk factors of dyslipidemia among academic staff and students in Bangladesh.
Keywords: Bangladesh; Dyslipidemia; Prevalence; Risk factors; University staff and students.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
Similar articles
-
Prevalence and factors associated with metabolic syndrome in university students and academic staff in Bangladesh.Sci Rep. 2023 Nov 14;13(1):19912. doi: 10.1038/s41598-023-46943-x. Sci Rep. 2023. PMID: 37963996 Free PMC article.
-
Prevalence and factors associated with dyslipidemia in Bangladeshi adults.PLoS One. 2023 Jan 20;18(1):e0280672. doi: 10.1371/journal.pone.0280672. eCollection 2023. PLoS One. 2023. PMID: 36662845 Free PMC article.
-
The relationship between dyslipidemia and inflammation among adults in east coast China: A cross-sectional study.Front Immunol. 2022 Aug 11;13:937201. doi: 10.3389/fimmu.2022.937201. eCollection 2022. Front Immunol. 2022. PMID: 36032093 Free PMC article.
-
Nutrition interventions for adults with dyslipidemia: A Clinical Perspective from the National Lipid Association.J Clin Lipidol. 2023 Jul-Aug;17(4):428-451. doi: 10.1016/j.jacl.2023.05.099. Epub 2023 Jun 2. J Clin Lipidol. 2023. PMID: 37271600 Review.
-
Obesity and Dyslipidemia.Curr Atheroscler Rep. 2023 Dec;25(12):947-955. doi: 10.1007/s11883-023-01167-2. Epub 2023 Nov 18. Curr Atheroscler Rep. 2023. PMID: 37979064 Review.
Cited by
-
Physical activity levels during COVID-19 pandemic and its associated factors in patients with Chagas disease.Front Med (Lausanne). 2024 Aug 6;11:1411977. doi: 10.3389/fmed.2024.1411977. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39165379 Free PMC article.
-
Evaluation of the relationship between xanthine oxidase activity and metabolic syndrome in a population group in Bangladesh.Sci Rep. 2024 Sep 2;14(1):20380. doi: 10.1038/s41598-024-71733-4. Sci Rep. 2024. PMID: 39223331 Free PMC article.
-
Evaluation of the Relationship Between Serum Uric Acid and Cardiovascular Disease: A Cross-Sectional Study in Bangladesh.Endocrinol Diabetes Metab. 2025 May;8(3):e70055. doi: 10.1002/edm2.70055. Endocrinol Diabetes Metab. 2025. PMID: 40312282 Free PMC article.
-
Prevalence and Mitigation of Cardiovascular Disease Risk Factors Among the Corporate Workforce in Sub-Saharan Africa: A Systematic Review and Meta-Analysis.Cureus. 2024 Dec 17;16(12):e75888. doi: 10.7759/cureus.75888. eCollection 2024 Dec. Cureus. 2024. PMID: 39822425 Free PMC article. Review.
-
Post-marketing quality assessment of some brands of rosuvastatin tablets available in Jos, North-Central Nigeria.BMC Chem. 2025 Apr 26;19(1):112. doi: 10.1186/s13065-025-01470-w. BMC Chem. 2025. PMID: 40287767 Free PMC article.
References
-
- McAloon CJ, Osman F, Glennon P, Lim PB, Hayat SA. Global epidemiology and incidence of Cardiovascular Disease. Cardiovascular Diseases. Elsevier; 2016. 57–96.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
