

Substitution of self-reported measures for objectively assessed grip strength and slow walk in the Physical Frailty Phenotype: ramifications for validity
- PMID: 37481528
- PMCID: PMC10362666
- DOI: 10.1186/s12877-023-04105-8
Substitution of self-reported measures for objectively assessed grip strength and slow walk in the Physical Frailty Phenotype: ramifications for validity
Abstract
Background: Frailty assessment promises to identify older adults at risk for adverse consequences following stressors and target interventions to improve health outcomes. The Physical Frailty Phenotype (PFP) is a widely-studied, well validated assessment but incorporates performance-based slow walk and grip strength criteria that challenge its use in some clinical settings. Variants replacing performance-based elements with self-reported proxies have been proposed. Our study evaluated whether commonly available disability self-reports could be substituted for the performance-based criteria in the PFP while still identifying as "frail" the same subpopulations of individuals.
Methods: Parallel analyses were conducted in 3393 female and 2495 male Cardiovascular Health Study, Round 2 participants assessed in 1989-90. Candidate self-reported proxies for the phenotype's "slowness" and "weakness" criteria were evaluated for comparable prevalence and agreement by mode of measurement. For best-performing candidates: Frailty status (3 + positive criteria out of 5) was compared for prevalence and agreement between the PFP and mostly self-reported versions. Personal characteristics were compared between those adjudicated as frail by (a) only a self-reported version; (b) only the PFP; (c) both, using bivariable analyses and multinomial logistic regression.
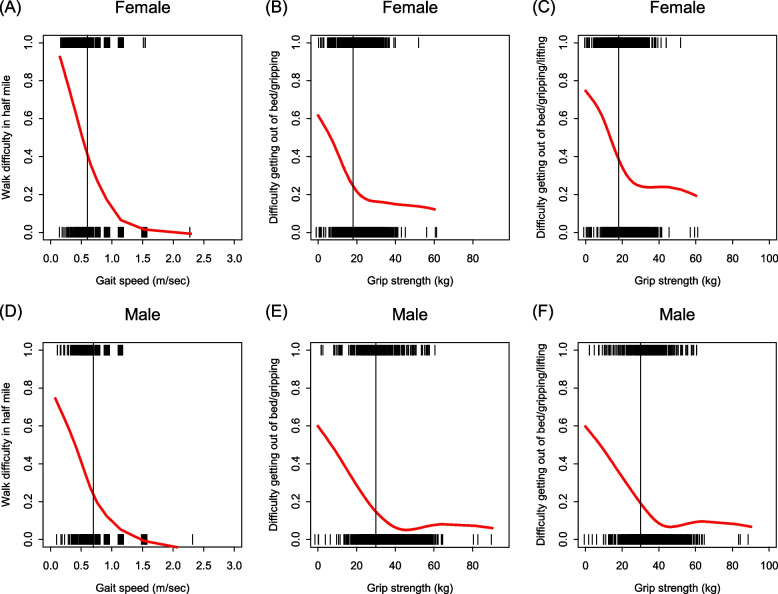
Results: Self-reported difficulty walking ½ mile was selected as a proxy for the phenotype's slowness criterion. Two self-reported weakness proxies were examined: difficulty transferring from a bed or chair or gripping with hands, and difficulty as just defined or in lifting a 10-pound bag. Prevalences matched to within 4% between self-reported and performance-based criteria in the whole sample, but in all cases the self-reported prevalence for women exceeded that for men by 11% or more. Cross-modal agreement was moderate, with by-criterion and frailty-wide Kappa statistics of 0.55-0.60 in all cases. Frail subgroups (a), (b), (c) were independently discriminated (p < 0.05) by race, BMI, and depression in women; by age in men; and by self-reported health for both.
Conclusions: Commonly used self-reported disability items cannot be assumed to stand in for performance-based criteria in the PFP. We found subpopulations identified as frail by resultant phenotypes versus the original phenotype to systematically differ. Work to develop self-reported proxies that more closely replicate their objective phenotypic counterparts than standard disability self-reports is needed.
Keywords: Aging; Construct validation; Diagnostic accuracy; Measurement error; Physical function; Vulnerability.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, Cesari M, Chumlea WC, Doehner W, Evans J, Fried LP, Guralnik JM, Katz PR, Malmstrom TK, McCarter RJ, Gutierrez Robledo LM, Rockwood K, von Haehling S, Vandewoude MF, Walston J. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14(6):392–397. doi: 10.1016/j.jamda.2013.03.022. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG023629/AG/NIA NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- P30 AG021334/AG/NIA NIH HHS/United States
- N01HC85082/HL/NHLBI NIH HHS/United States
- N01HC85086/HL/NHLBI NIH HHS/United States
- R03AG048541/AG/NIA NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01HC85079/HL/NHLBI NIH HHS/United States
- N01HC85083/HL/NHLBI NIH HHS/United States
- P30AG021334/AG/NIA NIH HHS/United States
- N01HC85081/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
