

Elevated blood and cerebrospinal fluid biomarkers of microglial activation and blood‒brain barrier disruption in anti-NMDA receptor encephalitis
- PMID: 37481571
- PMCID: PMC10363307
- DOI: 10.1186/s12974-023-02841-7
Elevated blood and cerebrospinal fluid biomarkers of microglial activation and blood‒brain barrier disruption in anti-NMDA receptor encephalitis
Abstract
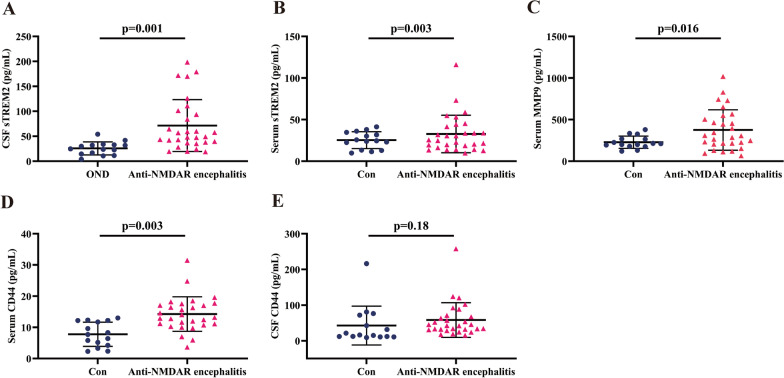
Background: Anti-NMDA receptor (NMDAR) encephalitis is an autoimmune disease characterized by complex neuropsychiatric syndrome and cerebrospinal fluid (CSF) NMDAR antibodies. Triggering receptor expressed on myeloid cells 2 (TREM2) has been reported to be associated with inflammation of the central nervous system (CNS). Matrix metalloproteinase-9 (MMP9) and cluster of differentiation (CD44) were measured to evaluate blood‒brain barrier (BBB) permeability in anti-NMDAR encephalitis. The roles of microglial activation and BBB disruption in anti-NMDAR encephalitis are not well known.
Findings: In this work, we detected increased expression levels of CSF sTREM2, CSF and serum CD44, and serum MMP9 in anti-NMDAR encephalitis patients compared with controls. CSF sTREM2 levels were positively related to both CSF CD44 levels (r = 0.702, p < 0.0001) and serum MMP9 levels (r = 0.428, p = 0.021). In addition, CSF sTREM2 levels were related to clinical parameters (modified Rankin Scale scores, r = 0.422, p = 0.023, and Glasgow Coma Scale scores, r = - 0.401, p = 0.031).
Conclusion: Increased sTREM2 levels in CSF as well as increased CD44 and MMP9 in serum and CSF reflected activation of microglia and disruption of the BBB in anti-NMDAR encephalitis, expanding the understanding of neuroinflammation in this disease. The factors mentioned above may have potential as novel targets for intervention or novel diagnostic biomarkers.
Keywords: Anti-NMDA receptor encephalitis; Blood‒brain barrier disruption; CD44; MMP9; Microglial activation; sTREM2.
© 2023. The Author(s).
Conflict of interest statement
All the authors declare that they have no potential competing interests concerning the research, authorship, and/or publication of this article.
Figures



References
-
- Titulaer MJ, McCracken L, Gabilondo I, Armangué T, Glaser C, Iizuka T, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013;12(2):157–165. doi: 10.1016/S1474-4422(12)70310-1. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
