

Adverse perinatal outcomes attributable to HIV in sub-Saharan Africa from 1990 to 2020: Systematic review and meta-analyses
- PMID: 37481594
- PMCID: PMC10363130
- DOI: 10.1038/s43856-023-00331-8
Adverse perinatal outcomes attributable to HIV in sub-Saharan Africa from 1990 to 2020: Systematic review and meta-analyses
Erratum in
-
Publisher Correction: Adverse perinatal outcomes attributable to HIV in sub-Saharan Africa from 1990 to 2020: systematic review and meta-analyses.Commun Med (Lond). 2023 Dec 12;3(1):180. doi: 10.1038/s43856-023-00415-5. Commun Med (Lond). 2023. PMID: 38086957 Free PMC article. No abstract available.
Abstract
Background: Maternal HIV infection and antiretroviral drugs (ARVs) are associated with increased risks of adverse perinatal outcomes. The vast majority of pregnant women living with HIV (WLHIV) reside in sub-Saharan Africa. We aimed to determine the burden of adverse perinatal outcomes attributable to HIV and ARVs in sub-Saharan Africa between 1990 and 2020.
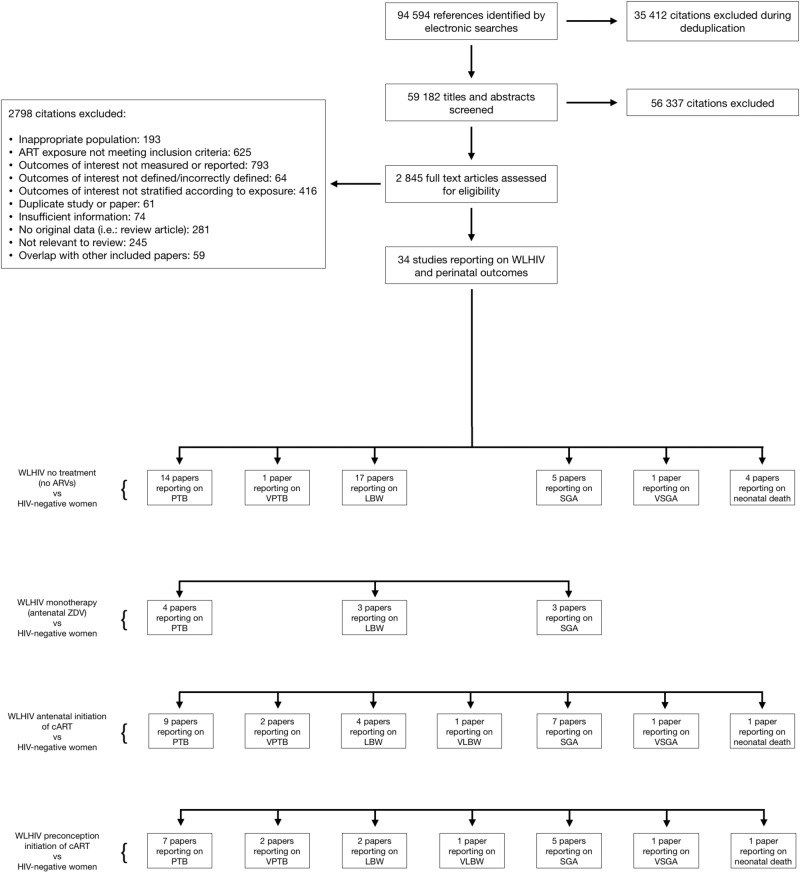
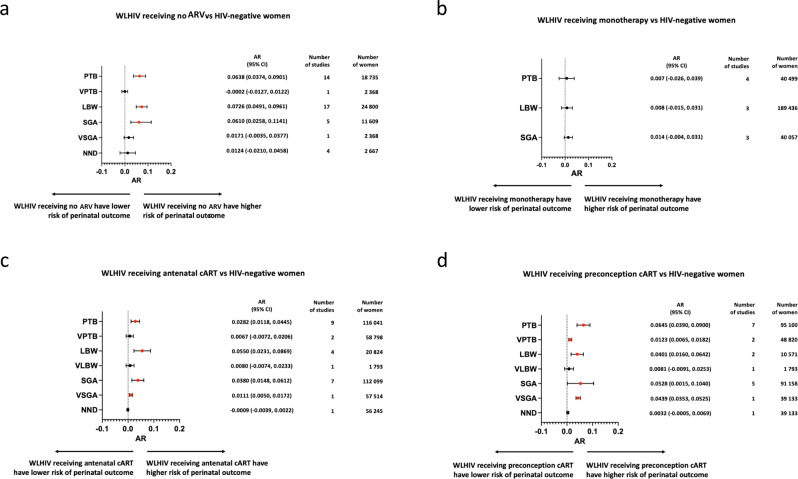
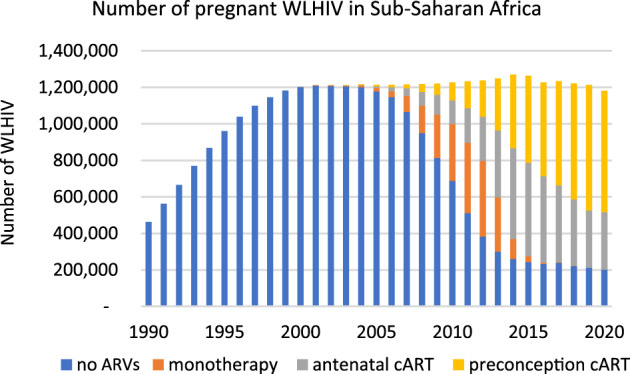
Methods: We conduct a systematic review of studies on the association of pregnant WLHIV with adverse perinatal outcomes in sub-Saharan Africa. We perform random-effects meta-analyses to determine the risk difference (attributable risk, AR) of perinatal outcomes among WLHIV receiving no ARVs, monotherapy, or combination antiretroviral therapy (cART) initiated antenatally or preconception, compared to HIV-negative women. We estimate numbers of perinatal outcomes attributable to HIV and ARVs by combining the AR values with numbers of WLHIV receiving different ARV regimens in each country in sub-Saharan Africa annually between 1990 and 2020.
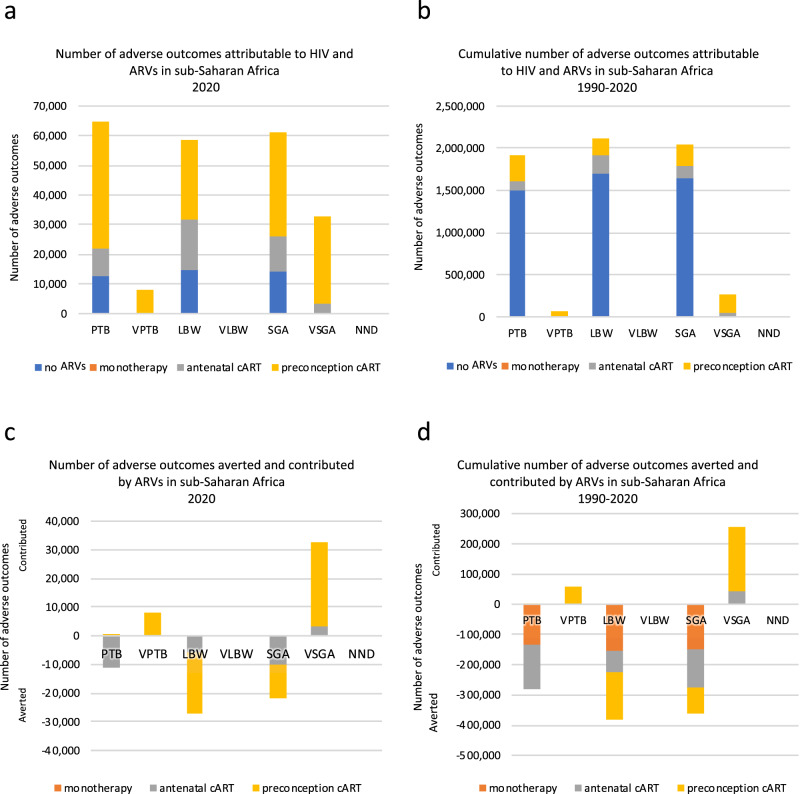
Results: We find that WLHIV receiving no ARVs or cART initiated antenatally or preconception, but not monotherapy, have an increased risk of preterm birth (PTB), low birthweight (LBW) and small for gestational age (SGA), compared to HIV-negative women. Between 1990 and 2020, 1,921,563 PTBs, 2,119,320 LBWs, and 2,049,434 SGAs are estimated to be attributable to HIV and ARVs in sub-Saharan Africa, mainly among WLHIV receiving no ARVs, while monotherapy and preconception and antenatal cART averted many adverse outcomes. In 2020, 64,585 PTBs, 58,608 LBWs, and 61,112 SGAs were estimated to be attributable to HIV and ARVs, the majority among WLHIV receiving preconception cART.
Conclusions: As the proportion of WLHIV receiving preconception cART increases, the burden of adverse perinatal outcomes among WLHIV in sub-Saharan Africa is likely to remain high.
Systematic review registration number: CRD42021248987.
Plain language summary
Pregnant women living with HIV (WLHIV) are at higher risk of adverse birth outcomes, such as babies born too soon (premature birth), babies born too small (low birthweight) or small-for-gestational-age (smaller than expected based on the weeks of pregnancy). It is unknown how many cases of these outcomes are attributable to HIV in sub-Saharan Africa, where most pregnant WLHIV reside. We conduct a search for published studies to determine the risk of adverse birth outcomes among WLHIV. We find that around 2 million premature births, low birthweight babies, and small-for-gestational-age babies are attributable to HIV in sub-Saharan Africa between 1990 and 2020. We conclude that adverse birth outcomes among WLHIV in sub-Saharan Africa are likely to remain high for the foreseeable future. Our findings could guide strategies to improve the health of WLHIV and their children in this region.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- United Nations. Transforming our world: The 2030 agenda for sustainable development. (2015).
-
- GBD. Under-5 Mortality Collaborators. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet. 2021;398:870–905. doi: 10.1016/S0140-6736(21)01207-1. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
