

Prediction of risk for myeloid malignancy in clonal hematopoiesis
- PMID: 37483562
- PMCID: PMC10361696
- DOI: 10.1056/evidoa2200310
Prediction of risk for myeloid malignancy in clonal hematopoiesis
Abstract
Background: Clonal hematopoiesis of indeterminate potential (CHIP) and clonal cytopenia of undetermined significance (CCUS) are defined by somatic mutations in genes associated with myeloid neoplasms (MN) at a variant allele fraction (VAF) ≥ 0.02, in the absence and presence of cytopenia, respectively. CHIP/CCUS is highly prevalent in adults and defining predictors of MN risk would aid clinical management and research.
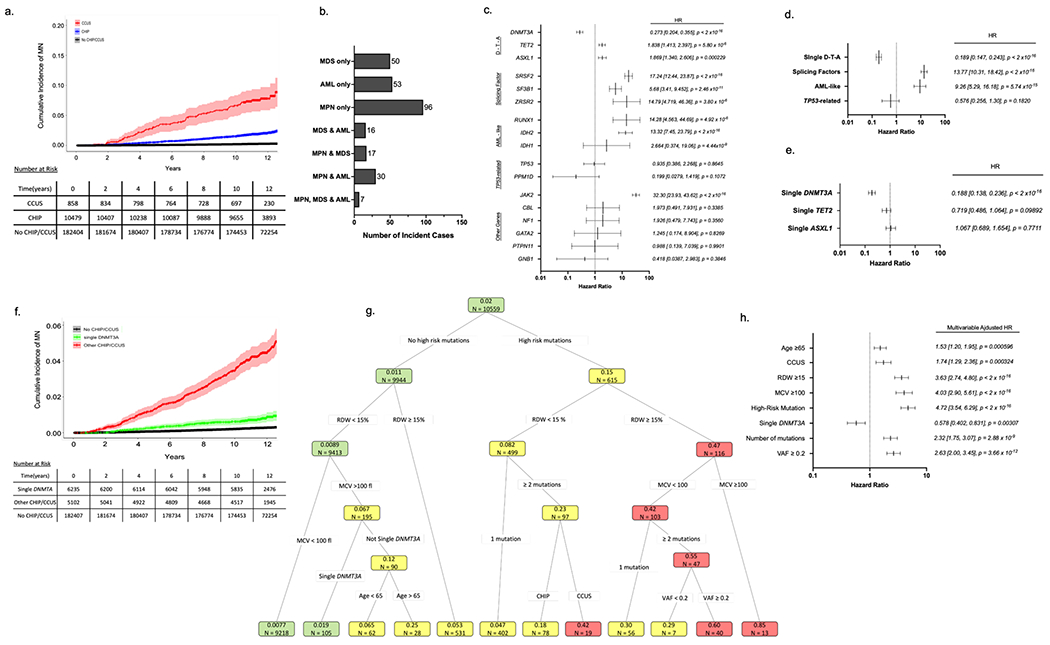
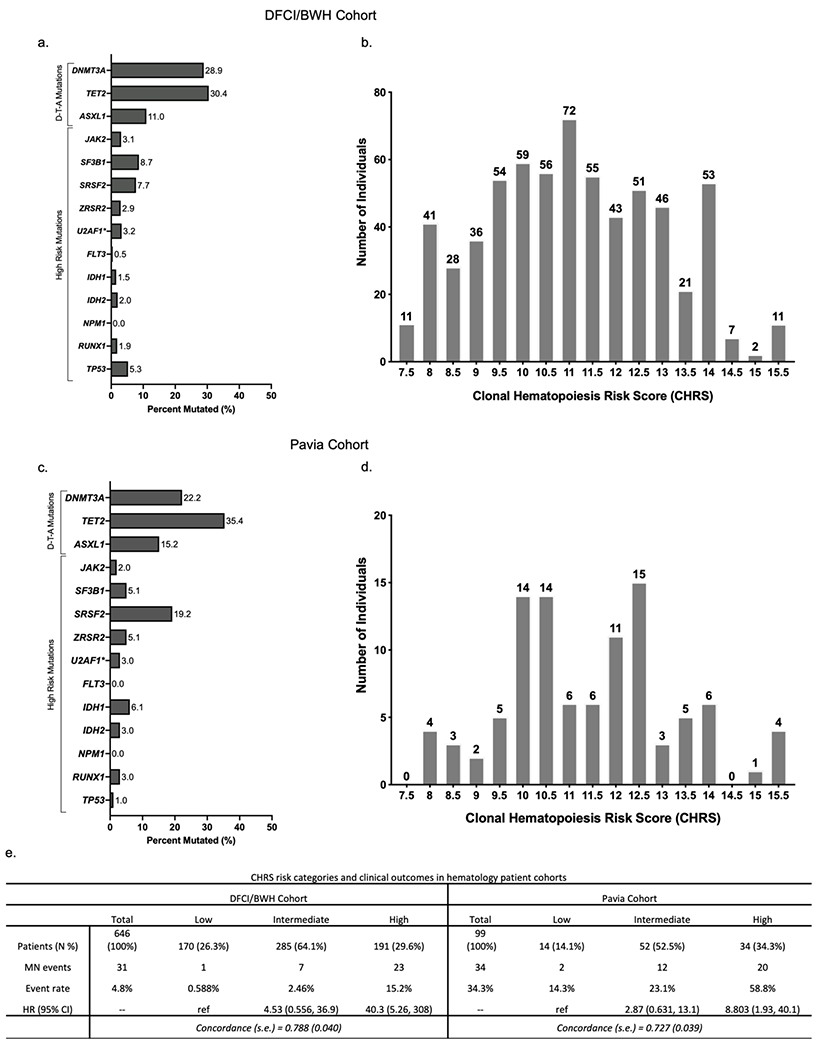
Methods: We analyzed sequenced exomes of healthy UK Biobank (UKB) participants (n = 438,890) in separate derivation and validation cohorts. Genetic mutations, laboratory values, and MN outcomes were used in conditional probability-based recursive partitioning and Cox regression to determine predictors of incident MN. Combined statistical weights defined a clonal hematopoiesis risk score (CHRS). Independent CHIP/CCUS patient cohorts were used to test prognostic capability of the CHRS in the clinical setting.
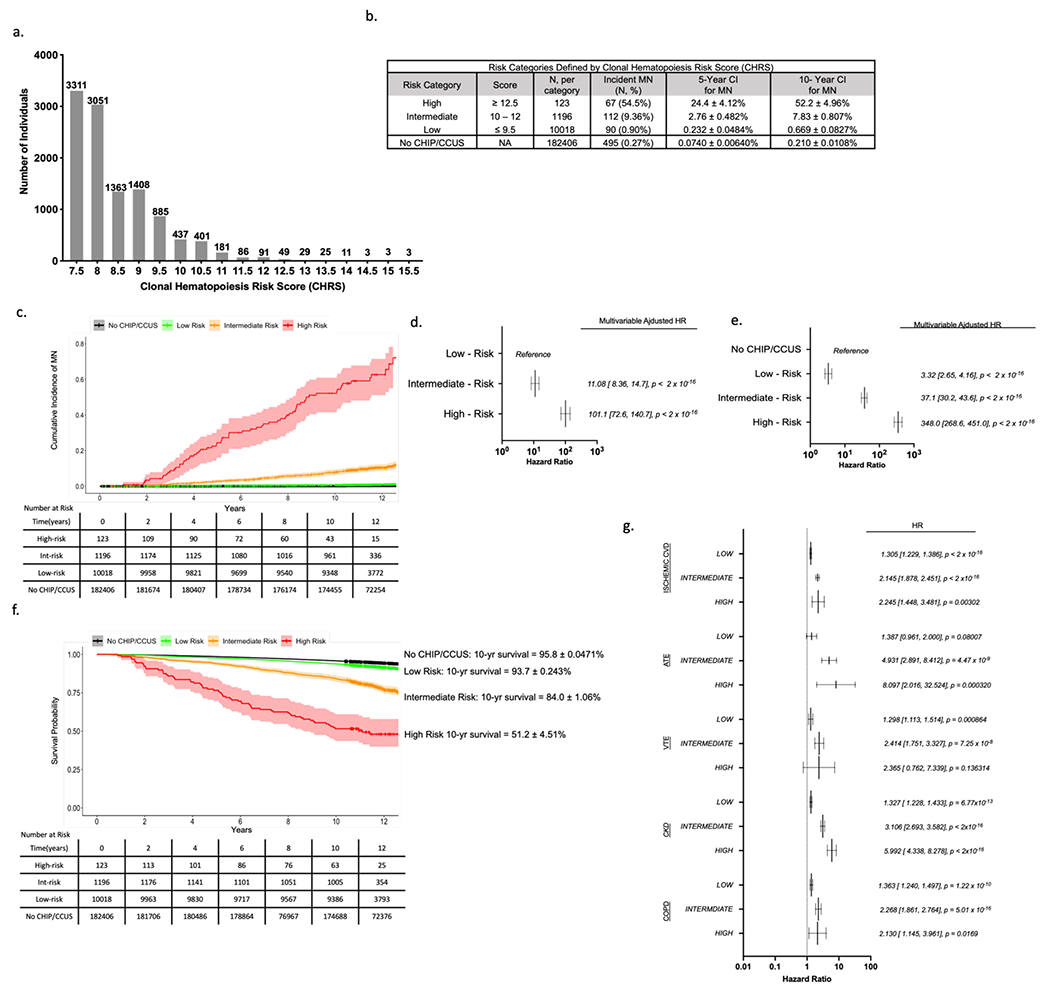
Results: Recursive partitioning distinguished CHIP/CCUS cases with 10-year probabilities of MN ranging from 0.0078 - 0.85. Multivariable analysis validated partitioning variables as predictors of MN. Key features, including single DNMT3A mutations, high risk mutations, ≥ 2 mutations, VAF ≥ 0.2, age ≥ 65 years, CCUS vs CHIP and red blood cell indices, influenced MN risk in variable direction. The CHRS defined low risk (n = 10018, 88.4%), intermediate risk (n = 1196, 10.5%), and high risk (n = 123, 1.1%) groups. In clinical cohorts, most MN events occurred in high risk CHIP/CCUS patients.
Conclusions: The CHRS provides simple prognostic framework for CHIP/CCUS, distinguishing a high risk minority from the majority of CHIP/CCUS which has minimal risk for progression to MN.
Conflict of interest statement
BLE has received research funding from Celgene, Deerfield, and Novartis and consulting fees from GRAIL. He serves on the scientific advisory boards for Skyhawk Therapeutics, Exo Therapeutics, and Neomorph Therapeutics and TenSixteen Bio, all unrelated to this work. DN is a current equity holder in Madrigal pharmaceuticals, unrelated to this work. ML has received research funding from Novartis and Abbvie and honoraria from Pfizer, all unrelated to this work. RCL has received consulting fees from bluebird bio, Takeda Pharmaceuticals, Qiagen, Nuprobe, and Thermo Fisher, all unrelated to this work. RMS reports grants from AbbVie, Agios, Arog, and Novartis and has received personal fees from AbbVie, Actinium, Agios, Argenx, Apteva, Astella, AstraZeneca, Biolinerx, Celgene, Daiichi-Sankyo, Elevate, Gemoab, Janssen, Jazz, Macrogenics, Novartis, Otsuka, Pfizer, Hoffman LaRoche, Stemline, Syndax, Syntrix, Syros, Takeda, and Trovagene, all unrelated to this work. DD has received research funding from Abbvie, Glycomimetics and Novartis as well as consulting fees from Blueprint Medicines, Incyte, Forty-Seven, Autolus, Agios, Amgen, Shire, Takeda, Novartis, Pfizer and Jazz, all unrelated to this work. RS is a member on the board of directors of Kladis, Be the Match/National Marrow Donor Program and Juno and has received personal fees from Alexion, Gilead, Rheos, Jazz and Vor Biopharma, all unrelated to this work. AGB is a current holder of stock options in TenSixteen Bio, unrelated to this work. SJ is a consultant to Novartis, AVRO Bio, Roche Genentech, and Foresite Labs, and is on the scientific advisory board and holds equity interest in TenSixteen Bio and Bitterroot Bio, all unrelated to this work. PN reports grant support from Amgen, Apple, AstraZeneca, Boston Scientific, and Novartis, personal fees from Apple, AstraZeneca, Blackstone Life Sciences, Genentech, and Novartis, advisory board participation and equity interest in TenSixteen Bio and spousal employment at Vertex, all unrelated to this work. The remaining authors declare no competing financial interests.
Figures
References
-
- Genovese G, Jaiswal S, Ebert BL, McCarroll SA. Clonal hematopoiesis and blood-cancer risk. N Engl J Med. 2015;372(11):1071–1072. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
