

The mechanisms and management of persistent postsurgical pain
- PMID: 37484030
- PMCID: PMC10357043
- DOI: 10.3389/fpain.2023.1154597
The mechanisms and management of persistent postsurgical pain
Abstract
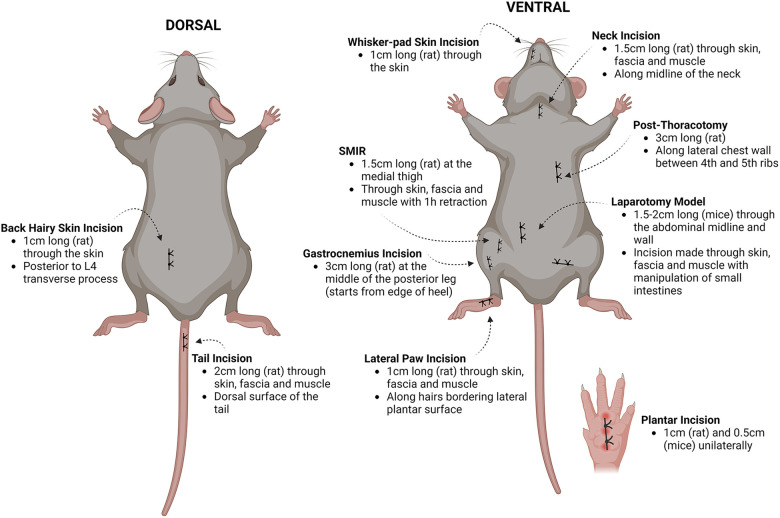
An estimated 10%-50% of patients undergoing a surgical intervention will develop persistent postsurgical pain (PPP) lasting more than 3 months despite adequate acute pain management and the availability of minimally invasive procedures. The link between early and late pain outcomes for surgical procedures remains unclear-some patients improve while others develop persistent pain. The elective nature of a surgical procedure offers a unique opportunity for prophylactic or early intervention to prevent the development of PPP and improve our understanding of its associated risk factors, such as pre-operative anxiety and the duration of severe acute postoperative pain. Current perioperative pain management strategies often include opioids, but long-term consumption can lead to tolerance, addiction, opioid-induced hyperalgesia, and death. Pre-clinical models provide the opportunity to dissect mechanisms underpinning the transition from acute to chronic, or persistent, postsurgical pain. This review highlights putative mechanisms of PPP, including sensitisation of peripheral sensory neurons, neuroplasticity in the central nervous system and nociceptive signalling along the neuro-immune axis.
Keywords: PPP; mechanisms; pre-clinical models; prevention; risks.
© 2023 Fuller, Bharde and Sikandar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Macrae W, Davies H. Epidemiology of pain. Core Top Pain. (1999) 99:125–42.
Publication types
LinkOut - more resources
Full Text Sources
Medical