

An impaired pituitary-adrenal signalling axis in stable cirrhosis is linked to worse prognosis
- PMID: 37484210
- PMCID: PMC10362733
- DOI: 10.1016/j.jhepr.2023.100789
An impaired pituitary-adrenal signalling axis in stable cirrhosis is linked to worse prognosis
Abstract
Background & aims: Inadequate adrenal function has been described in patients with cirrhosis. We investigated (i) the pituitary-adrenal axis at different clinical stages and (ii) the clinical impact of decreased serum cortisol levels in stable patients with advanced chronic liver disease (ACLD).
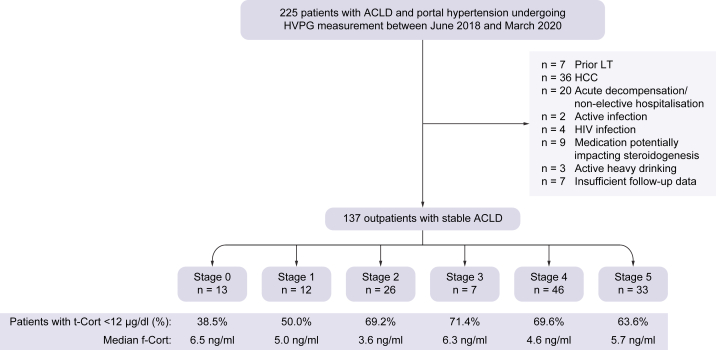
Methods: We included 137 outpatients with ACLD undergoing hepatic venous pressure gradient (HVPG) measurement in the prospective VICIS study (NCT03267615). Patients were stratified into six clinical stages: S0: subclinical portal hypertension (PH) (HVPG 6-9 mmHg), S1: clinically significant PH (HVPG ≥10 mmHg) without varices, S2: presence of varices, S3: previous variceal bleeding, S4: previous non-bleeding decompensation, and S5: further decompensation.
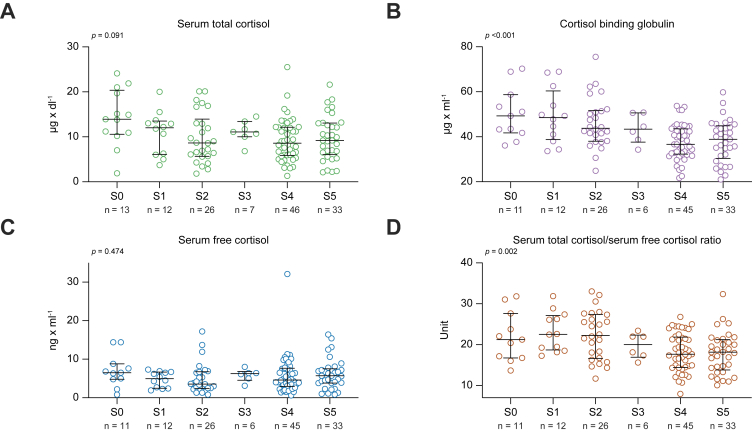
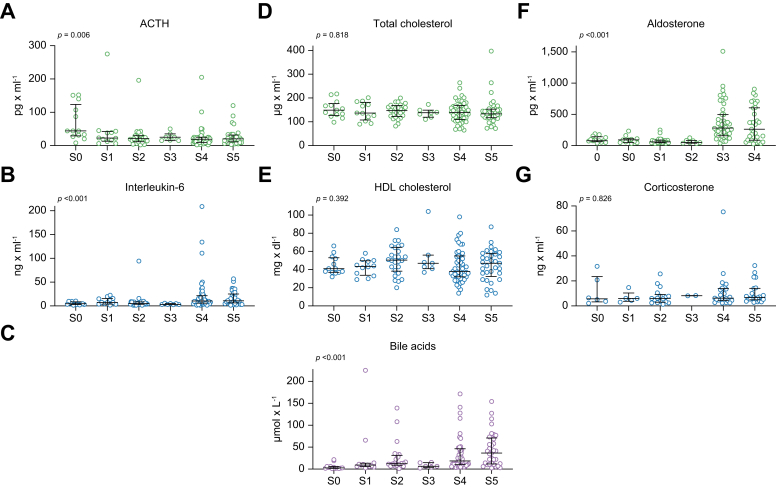
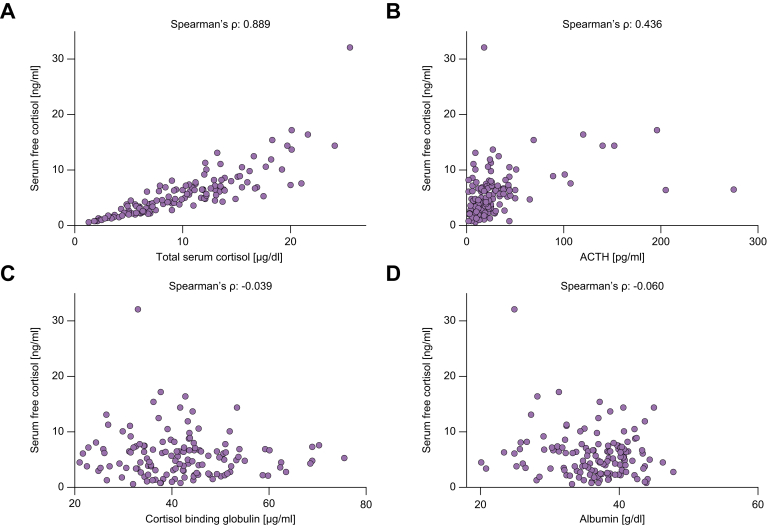
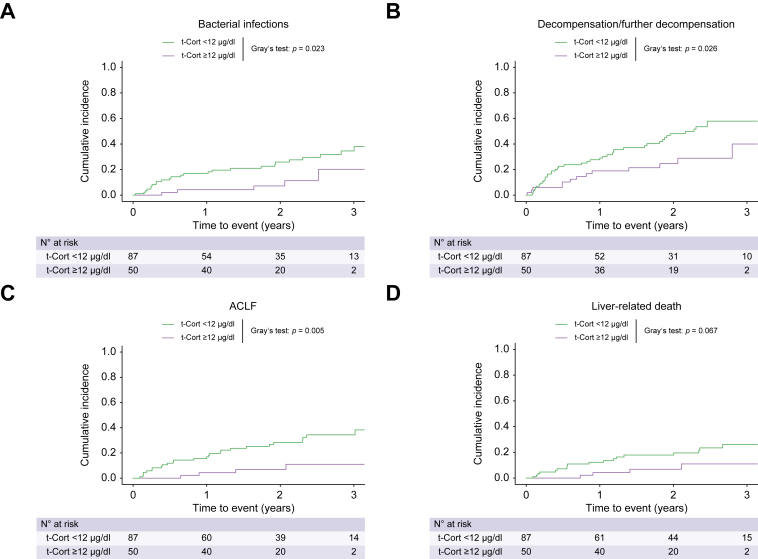
Results: Fifty-one patients had compensated ACLD (S0: n = 13; S1: n = 12; S2: n = 26), whereas 86 patients had decompensated ACLD (S3: n = 7; S4: n = 46; S5: n = 33). Serum total cortisol (t-Cort) showed a strong correlation with estimated serum free cortisol (f-Cort; Spearman's ρ: 0.889). With progressive clinical stage, median ACTH levels (from S0: 44.0 pg/ml to S5: 20.0 pg/ml; p = 0.006), t-Cort (from S0: 13.9 μg/dl to S5: 9.2 μg/dl; p = 0.091), and cortisol binding globulin (from S0: 49.3 μg/ml to S5: 38.9 μg/ml; p <0.001) decreased, whereas f-Cort (p = 0.474) remained unchanged. Lower t-Cort levels independently predicted bacterial infections (asHR: 1.11; 95% CI: 1.04-1.19; p = 0.002), further decompensation (asHR: 1.08; 95% CI: 1.02-1.12; p = 0.008), acute-on-chronic liver failure (ACLF; asHR: 1.11; 95% CI: 1.04-1.19; p = 0.002), and liver-related death (asHR: 1.09; 95% CI: 1.01-1.18; p = 0.045).
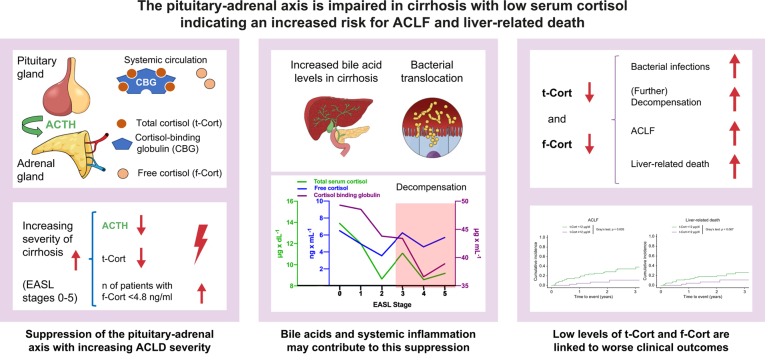
Conclusions: The pituitary-ACTH-adrenal-cortisol axis is progressively suppressed with increasing severity of cirrhosis. Lower t-Cort is an independent risk factor for bacterial infections, further decompensation of ACLF, and liver-related mortality-even in stable outpatients with cirrhosis.
Clinical trial number: Vienna Cirrhosis Study (VICIS; NCT: NCT03267615).
Impact and implications: In a cohort of stable outpatients, we observed progressive suppression of the pituitary-adrenal axis with increasing clinical stage of advanced chronic liver disease (ACLD). Increased levels of bile acids and systemic inflammation (assessed by interleukin-6 levels) could be involved in this suppression. Serum total cortisol (t-Cort) was strongly correlated with serum free cortisol (f-Cort) and lower t-Cort levels were independently associated with a higher risk of adverse clinical outcomes, including bacterial infections, further decompensation, acute-on-chronic liver failure, and liver-related death.
Keywords: ACTH; Advanced chronic liver disease; Bile acids; Cirrhosis; Cortisol; Inflammation; Non-invasive testing; Portal hypertension.
© 2023 The Authors.
Conflict of interest statement
The authors have nothing to disclose regarding the work under consideration for publication. Conflicts of interests outside the submitted work: LH, MJ, PW, LB, GS, MS, and RM have nothing to disclose. BSim. received travel support from AbbVie and Gilead. DJMB received speaker fees from AbbVie and Siemens, as well as grant support form Gilead and Siemens, as well as travel support from AbbVie and Gilead. BSch. received travel support from AbbVie, Ipsen, and Gilead. MT served as a speaker and/or consultant and/or advisory board member for Albireo, BiomX, Falk, Boehringer Ingelheim, Bristol-Myers Squibb, Falk, Genfit, Gilead, Intercept, Janssen, MSD, Novartis, Phenex, Pliant, Regulus, and Shire, and received travel support from AbbVie, Falk, Gilead, and Intercept, as well as grants/research support from Albireo, Alnylam, Cymabay, Falk, Gilead, Intercept, MSD, Takeda, and UltraGenyx. He is also co-inventor of patents on the medical use of 24-norursodeoxycholic acid. MM served as a speaker and/or consultant and/or advisory board member for AbbVie, Collective Acumen, Gilead, Takeda, and W. L. Gore & Associates and received travel support from AbbVie and Gilead. TR served as a speaker and/or consultant and/or advisory board member for AbbVie, Bayer, Boehringer Ingelheim, Gilead, Intercept, MSD, Siemens, and W. L. Gore & Associates and received grants/research support from AbbVie, Boehringer Ingelheim, Gilead, Intercept, MSD, Myr Pharmaceuticals, Pliant, Philips, Siemens, and W. L. Gore & Associates as well as travel support from AbbVie, Boehringer Ingelheim, Gilead and Roche. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Similar articles
-
Lower free triiodothyronine (fT3) levels in cirrhosis are linked to systemic inflammation, higher risk of acute-on-chronic liver failure, and mortality.JHEP Rep. 2023 Nov 1;6(1):100954. doi: 10.1016/j.jhepr.2023.100954. eCollection 2024 Jan. JHEP Rep. 2023. PMID: 38125301 Free PMC article.
-
Systemic inflammation increases across distinct stages of advanced chronic liver disease and correlates with decompensation and mortality.J Hepatol. 2021 Apr;74(4):819-828. doi: 10.1016/j.jhep.2020.10.004. Epub 2020 Oct 16. J Hepatol. 2021. PMID: 33075344
-
Insulin-like growth factor-1 in cirrhosis is linked to hepatic dysfunction and fibrogenesis and predicts liver-related mortality.Aliment Pharmacol Ther. 2025 Jan;61(1):88-98. doi: 10.1111/apt.18289. Epub 2024 Sep 21. Aliment Pharmacol Ther. 2025. PMID: 39305115 Free PMC article.
-
Approaches to the Diagnosis of Portal Hypertension: Non-Invasive or Invasive Tests?Hepat Med. 2021 Mar 18;13:25-36. doi: 10.2147/HMER.S278077. eCollection 2021. Hepat Med. 2021. PMID: 33776492 Free PMC article. Review.
-
[Evaluation and treatment of portal hypertension].Cas Lek Cesk. 2016;155(2):22-6. Cas Lek Cesk. 2016. PMID: 27088788 Review. Czech.
Cited by
-
Low Urinary Free Cortisol as a Risk Factor for Patients with Variceal Bleeding.Medicina (Kaunas). 2023 Dec 2;59(12):2112. doi: 10.3390/medicina59122112. Medicina (Kaunas). 2023. PMID: 38138215 Free PMC article.
-
Lower free triiodothyronine (fT3) levels in cirrhosis are linked to systemic inflammation, higher risk of acute-on-chronic liver failure, and mortality.JHEP Rep. 2023 Nov 1;6(1):100954. doi: 10.1016/j.jhepr.2023.100954. eCollection 2024 Jan. JHEP Rep. 2023. PMID: 38125301 Free PMC article.
-
Artificial intelligence-based evaluation of prognosis in cirrhosis.J Transl Med. 2024 Oct 14;22(1):933. doi: 10.1186/s12967-024-05726-2. J Transl Med. 2024. PMID: 39402630 Free PMC article. Review.
-
Joint Group and Multi Institutional Position Opinion: Cirrhotic Cardiomyopathy-From Fundamentals to Applied Tactics.Medicina (Kaunas). 2024 Dec 31;61(1):46. doi: 10.3390/medicina61010046. Medicina (Kaunas). 2024. PMID: 39859028 Free PMC article. Review.
-
Decreasing interleukin-6 levels after TIPS predict outcomes in decompensated cirrhosis.JHEP Rep. 2024 Dec 18;7(4):101308. doi: 10.1016/j.jhepr.2024.101308. eCollection 2025 Apr. JHEP Rep. 2024. PMID: 40124165 Free PMC article.
References
-
- Sepanlou S.G., Safiri S., Bisignano C., Ikuta K.S., Merat S., Saberifiroozi M., et al. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5:245–266. - PMC - PubMed
-
- D'Amico G., Garcia-Tsao G., Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44:217–231. - PubMed
-
- Costa D., Simbrunner B., Jachs M., Hartl L., Bauer D., Paternostro R., et al. Systemic inflammation increases across distinct stages of advanced chronic liver disease and correlates with decompensation and mortality. J Hepatol. 2021;74:819–828. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
