

Integrating the autoimmune connective tissue diseases for the medical student: A classification proposal based on pathogenesis and clinical phenotype
- PMID: 37484370
- PMCID: PMC10361038
- DOI: 10.1016/j.heliyon.2023.e16935
Integrating the autoimmune connective tissue diseases for the medical student: A classification proposal based on pathogenesis and clinical phenotype
Abstract
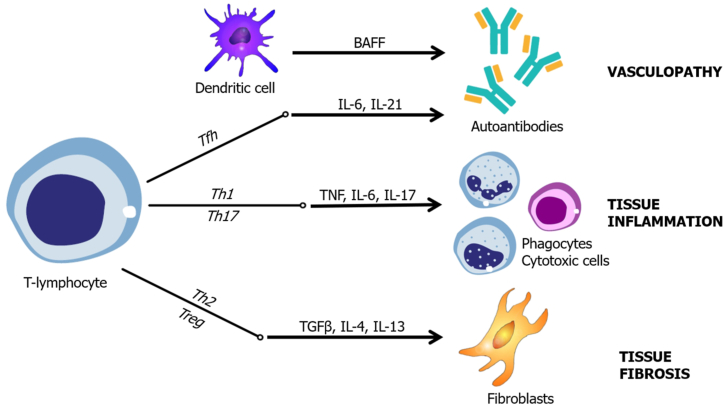
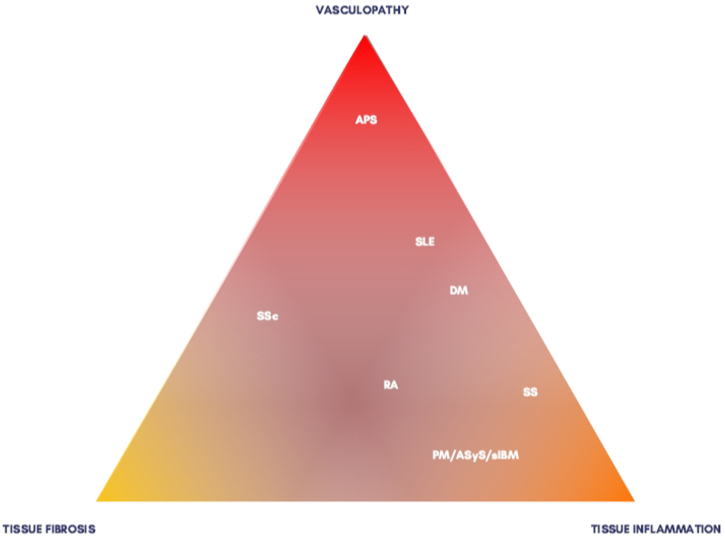
It is hard for medical students to recognize and understand the clinical presentation of systemic connective tissue diseases (SCTDs). In this study, we aimed to review the immune mechanisms of the main SCTDs and to propose a classification system focused on the student and based on each immune dysfunction's clinical phenotype. The search involved the MEDLINE database and included the terms "systemic lupus erythematosus," "antiphospholipid syndrome," "inflammatory myopathies," "rheumatoid arthritis," "Sjögren's syndrome" or "systemic sclerosis" and "pathogenesis," and "immunology" or "mechanism of disease." Systemic lupus erythematosus (SLE) is a prototypic immune-complex disease with a tendency toward vascular injury. Antiphospholipid syndrome (APS) is a diffuse immune-mediated thrombotic vasculopathy. In inflammatory myopathies (IMs), muscle inflammation leading to muscle weakness is the cardinal manifestation. Rheumatoid arthritis (RA) is a unique form of erosive and destructive polyarthritis. Sjögren's syndrome (SS) causes sicca symptoms due to infiltration of the exocrine glands. Disseminated fibrosis in systemic sclerosis (SSc) is caused by vascular injury with excessive fibroblast activation. After the review, we created a focus group involving all the authors to group the diseases according to their pathogenesis and clinical phenotype. Our group agreed that SCTDs can be divided in 3 groups based on the preferential clinical presentation and immune dysfunction: 1) vasculopathic features (SLE and APS), 2) tissue inflammation (IMs, RA, and SS), and 3) tissue fibrosis (SSc). In synthesis, we suggest that clustering SCTDs in groups based on clinical phenotype and presumptive immune dysfunction instead of ordering autoantibodies randomly can help students understand the diseases.
Keywords: Connective tissue diseases; Immunology; Medical students; Pathogenesis; Teaching.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper
Figures
References
-
- McCarthy E.M., Sheane B.J., Cunnane G. Greater focus on clinical rheumatology is required for training in internal medicine. Clin. Rheumatol. 2009;28:139–143. - PubMed
-
- Katz S.J., Oswald A.E. How confident are internal medicine residents in rheumatology versus other common internal medicine clinical skills: an issue of training time or exposure? Clin. Rheumatol. 2011;30:1081–1093. - PubMed
-
- West S.G., Kolfenbach J. fourth ed. Elsevier; Philadelphia: 2020. Rheumatology Secrets; pp. 118–218.
-
- Hochberg M. seventh ed. Elsevier; Philadelphia: 2019. Rheumatology; pp. 1103–1127.
-
- Kaul A., Gordon C., Crow M.K., et al. Systemic lupus erythematosus. Nat. Rev. Dis. Prim. 2016;2 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
