

Changes in low-acuity patient volume in an emergency department after launching a walk-in clinic
- PMID: 37484497
- PMCID: PMC10361543
- DOI: 10.1002/emp2.13011
Changes in low-acuity patient volume in an emergency department after launching a walk-in clinic
Abstract
Objective: Unscheduled low-acuity care options are on the rise and are often expected to reduce emergency department (ED) visits. We opened an ED-staffed walk-in clinic (WIC) as an alternative care location for low-acuity patients at a time when ED visits exceeded facility capacity and the impending flu season was anticipated to increase visits further, and we assessed whether low-acuity ED patient visits decreased after opening the WIC.
Methods: In this retrospective cohort study, we compared patient and clinical visit characteristics of the ED and WIC patients and conducted interrupted time-series analyses to quantify the impact of the WIC on low-acuity ED patient visit volume and the trend.
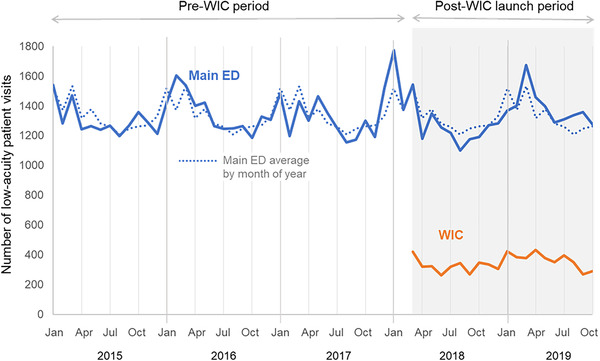
Results: There were 27,211 low-acuity ED visits (22.7% of total ED visits), and 7,058 patients seen in the WIC from February 26, 2018, to November 17, 2019. Low-acuity patient visits in the ED reduced significantly immediately after the WIC opened (P = 0.01). In the subsequent months, however, patient volume trended back to pre-WIC volumes such that there was no significant impact at 6, 9, or 12 months (P = 0.07). Had WIC patients been seen in the main ED, low-acuity volume would have been 27% of the total volume rather than the 22.7% that was observed.
Conclusion: The WIC did not result in a sustained reduction in low-acuity patients in the main ED. However, it enabled emergency staff to see low-acuity patients in a lower resource setting during times when ED capacity was limited.
Keywords: care use; clinical operations; emergency department; emergency department census; emergency department overcrowding; emergency department patient volume; low‐acuity; unscheduled care; urgent care; walk‐in clinic.
© 2023 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources
