

Short- and long-term safety and efficacy of corneal collagen cross-linking in progressive keratoconus: A systematic review and meta-analysis of randomized controlled trials
- PMID: 37484615
- PMCID: PMC10361434
- DOI: 10.4103/2211-5056.361974
Short- and long-term safety and efficacy of corneal collagen cross-linking in progressive keratoconus: A systematic review and meta-analysis of randomized controlled trials
Abstract
Purpose: The purpose of the study is to evaluate the safety and outcomes of corneal collagen cross-linking (CXL) and different CXL protocols in progressive keratoconus (PK) population at short and long-term.
Materials and methods: A systematic review and meta-analysis was conducted. A total of eight literature databases were searched (up to February 15, 2022). Randomized controlled trials (RCTs) comparing CXL versus placebo/control or comparing different CXL protocols in the PK population were included. The primary objective was assessment of outcomes of CXL versus placebo and comparison of different CXL protocols in terms of maximum keratometry (Kmax) or Kmax change from baseline (Δ), spherical equivalent, best corrected visual acuity (BCVA), and central corneal thickness (CCT) in both at short term (6 months) and long term (1st, 2nd, and 3rd year or more). The secondary objective was comparative evaluation of safety. For the meta-analysis, the RevMan5.3 software was used.
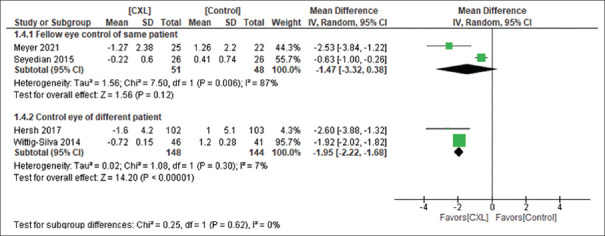
Results: A total of 48 RCTs were included. Compared to control, CXL was associated with improvement in Δ Kmax at 1 year (4 RCTs, mean difference [MD], -1.78 [-2.71, -0.86], P = 0.0002) and 2 and 3 years (1 RCT); ΔBCVA at 1 year (7 RCTs, -0.10 [-0.14, -0.06], P < 0.00001); and Δ CCT at 1 year (2 RCTs) and 3 years (1 RCT). Compared to conventional CXL (C-CXL), deterioration in Δ Kmax, ΔBCVA and endothelial cell density was seen at long term in the transepithelial CXL (TE-CXL, chemical enhancer). Up to 2 years, there was no difference between TE-CXL using iontophoresis (T-ionto) and C-CXL. At 2 and 4 years, C-CXL performed better compared to accelerated CXL (A-CXL) in terms of improving Kmax. Although CCT was higher in the A-CXL arm at 2 years, there was no difference at 4 years. While exploring heterogeneity among studies, selection of control eye (fellow eye of the same patient vs. eye of different patient) and baseline difference in Kmax were important sources of heterogeneity.
Conclusion: CXL outperforms placebo/control in terms of enhancing Kmax and CCT, as well as slowing disease progression over time (till 3 years). T-ionto protocol, on the other hand, performed similarly to C-CXL protocol up to 2 years.
Keywords: Collagen cross-linking; cornea; cross-linking; keratoconus; progressive keratoconus.
Copyright: © 2022 Taiwan J Ophthalmol.
Conflict of interest statement
The authors declare that there are no conflicts of interests of this paper.
Figures



References
-
- Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322. - PubMed
-
- Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous