

Revisiting the central aortopulmonary shunt procedure
- PMID: 37484647
- PMCID: PMC10357854
- DOI: 10.5606/tgkdc.dergisi.2023.24247
Revisiting the central aortopulmonary shunt procedure
Abstract
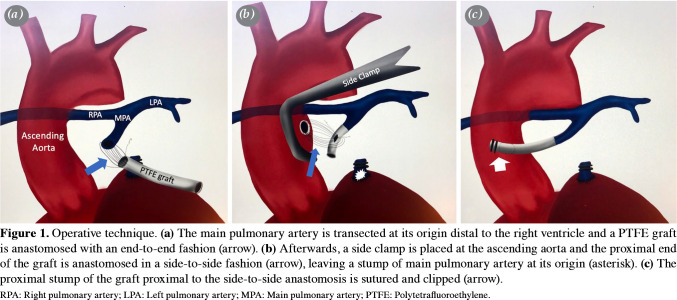
Background: In this study, we present our experience with the central aortopulmonary shunt technique with interposing a polytetrafluoroethylene graft between main pulmonary artery (end-to-end) and the ascending aorta (side-to-side) in a variety of cyanotic congenital heart defects.
Methods: Between January 2019 and June 2022, a total of 10 patients (6 males, 4 females; mean age: 4.3±2.8 months; range, 5 days to 10 months) with hypoplastic central pulmonary arteries who underwent central aortopulmonary shunt procedure were retrospectively analyzed. Demographic characteristics, preoperative, operative, and postoperative data of the patients were recorded. The Nakata indices of the patients were also noted before the procedure, as well as before the second stage of palliation or definitive repair.
Results: Four (40%) patients were operated as the first-step palliation for univentricular circulation. Six (60%) patients had well-developed ventricles and were palliated to be treated with total correction. The median follow-up after the procedure was 12 (range, 8 to 16) months. The mean systemic arterial saturation level at room air was 89.3±2.9% during follow-up. No mortality was observed in any patient.
Conclusion: A central aortopulmonary shunt procedure provides a reliable antegrade blood flow with a relatively non-challenging surgical technique that offers sufficient growth for the hypoplastic and confluent central pulmonary arteries with a very low risk of shunt thrombosis and overflow.
Keywords: Cardiac; congenital heart disease; pulmonary artery; pulmonary vein; shunt.
Copyright © 2023, Turkish Society of Cardiovascular Surgery.
Conflict of interest statement
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Figures

References
-
- Sumacker HB Jr, Mandelbaum I. Ascending aorticpulmonary artery shunts in cyanotic heart disease. Surgery. 1962;52:675–678. - PubMed
-
- Barragry TP, Ring WS, Blatchford JW, Foker JE. Central aorta-pulmonary artery shunts in neonates with complex cyanotic congenital heart disease. J Thorac Cardiovasc Surg. 1987;93:767–774. - PubMed
LinkOut - more resources
Full Text Sources