

Accuracy Evaluation Trial of Mixed Reality-Guided Spinal Puncture Technology
- PMID: 37484696
- PMCID: PMC10361284
- DOI: 10.2147/TCRM.S416918
Accuracy Evaluation Trial of Mixed Reality-Guided Spinal Puncture Technology
Abstract
Purpose: To evaluate the accuracy of mixed reality (MR)-guided visualization technology for spinal puncture (MRsp).
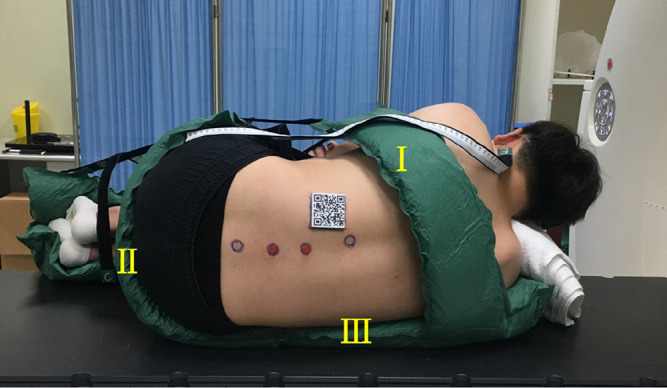
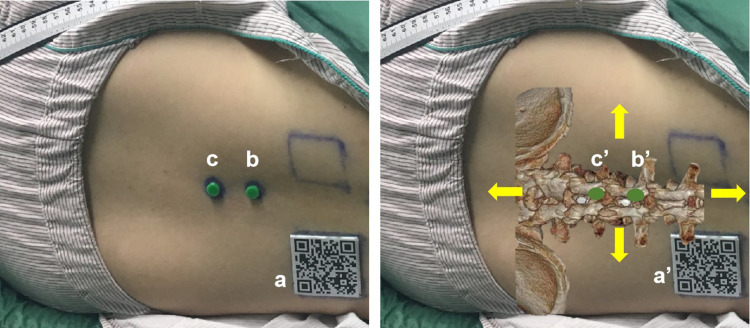
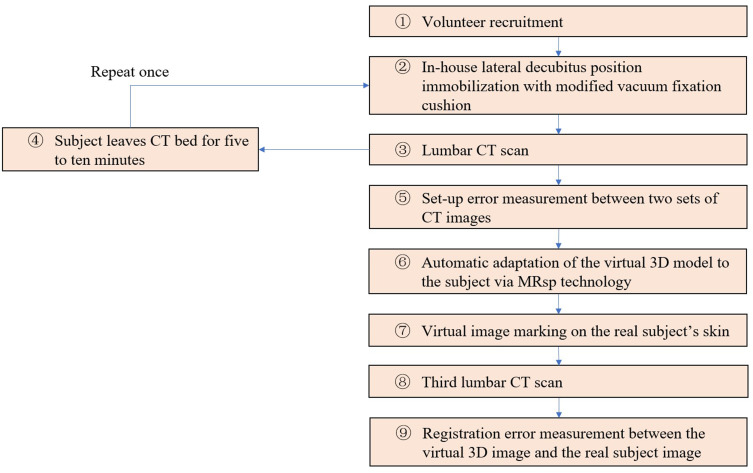
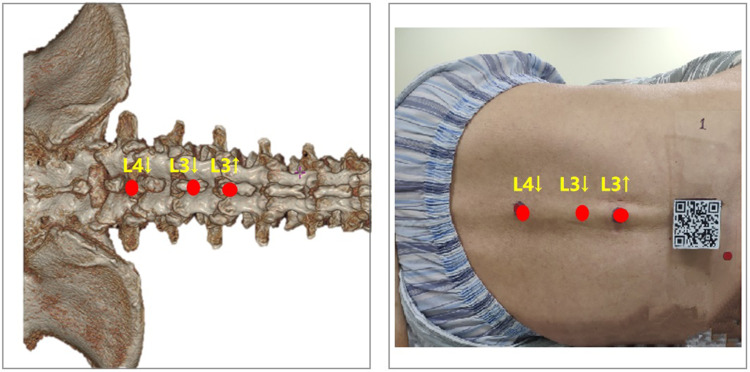
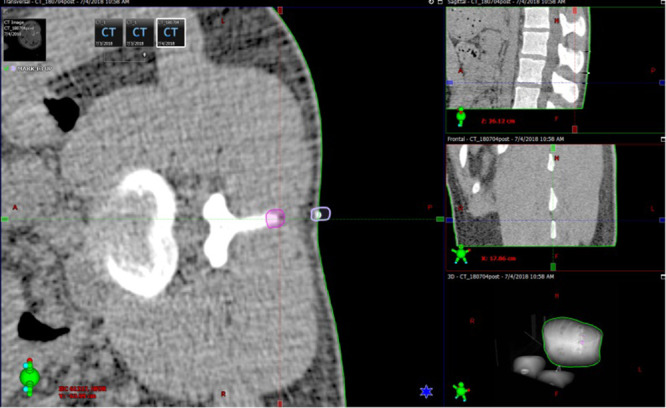
Methods: MRsp involved the following three steps: 1. Lumbar spine computed tomography (CT) data were obtained to reconstruct virtual 3D images, which were imported into a HoloLens (2nd gen). 2. The patented MR system quickly recognized the spatial orientation and superimposed the virtual image over the real spine in the HoloLens. 3. The operator performed the spinal puncture with structural information provided by the virtual image. A posture fixation cushion was used to keep the subjects' lateral decubitus position consistent. 12 subjects were recruited to verify the setup error and the registration error. The setup error was calculated using the first two CT scans and measuring the displacement of two location markers. The projection points of the upper edge of the L3 spinous process (L3↑), the lower edge of the L3 spinous process (L3↓), and the lower edge of the L4 spinous process (L4↓) in the virtual image were positioned and marked on the skin as the registration markers. A third CT scan was performed to determine the registration error by measuring the displacement between the three registration markers and the corresponding real spinous process edges.
Results: The setup errors in the position of the cranial location marker between CT scans along the left-right (LR), anterior-posterior (AP), and superior-inferior (SI) axes of the CT bed measured 0.09 ± 0.06 cm, 0.30 ± 0.28 cm, and 0.22 ± 0.12 cm, respectively, while those of the position of the caudal location marker measured 0.08 ± 0.06 cm, 0.29 ± 0.18 cm, and 0.18 ± 0.10 cm, respectively. The registration errors between the three registration markers and the subject's real L3↑, L3↓, and L4↓ were 0.11 ± 0.09 cm, 0.15 ± 0.13 cm, and 0.13 ± 0.10 cm, respectively, in the SI direction.
Conclusion: This MR-guided visualization technology for spinal puncture can accurately and quickly superimpose the reconstructed 3D CT images over a real human spine.
Keywords: immobilization; mixed reality; registration error; setup error; spinal puncture; superimposition.
© 2023 Wu et al.
Conflict of interest statement
The authors declare no conflicts of interest in this work.
Figures


References
-
- Stubbs BM, Badcock KJM, Hyams C, Rizal FE, Warren S, Francis D. A prospective study of early removal of the urethral catheter after colorectal surgery in patients having epidural analgesia as part of the Enhanced Recovery After Surgery programme. Colorectal Dis. 2013;15:733–736. doi:10.1111/codi.12124 - DOI - PubMed
LinkOut - more resources
Full Text Sources
