

Cutaneous lesions and other non-endocrine manifestations of Multiple Endocrine Neoplasia type 1 syndrome
- PMID: 37484956
- PMCID: PMC10360178
- DOI: 10.3389/fendo.2023.1191040
Cutaneous lesions and other non-endocrine manifestations of Multiple Endocrine Neoplasia type 1 syndrome
Abstract
Background: Multiple Endocrine Neoplasia type 1 is a rare genetic syndrome mainly caused by mutations of MEN1 gene and characterized by a combination of several endocrine and non-endocrine manifestations. The objective of this study was to describe cutaneous lesions and other non-endocrine manifestations of MEN1 in a cohort of patients with familial (F) and sporadic (S) MEN1, compare the prevalence of these manifestations between the two cohorts, and investigate the correlation with MEN1 mutation status.
Methods: We collected phenotypic and genotypic data of 185 patients with F-MEN1 and S-MEN1 followed from 1997 to 2022. The associations between F-MEN1 and S-MEN1 or MEN1 mutation-positive and mutation-negative patients and non-endocrine manifestations were determined using chi-square or Fisher's exact tests or multivariate exact logistic regression analyses.
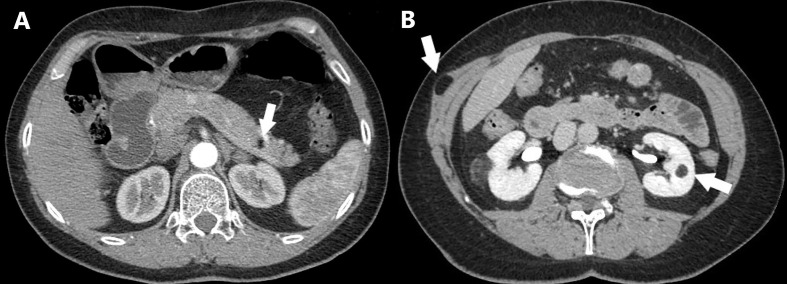
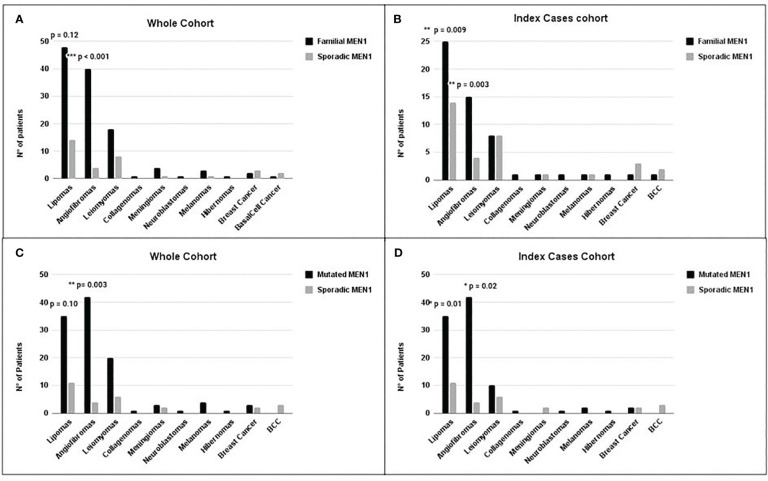
Results: The prevalence of angiofibromas was significantly higher in F-MEN1 than in S-MEN1 in both the whole (p < 0.001) and index case (p = 0.003) cohorts. The prevalence of lipomas was also significantly higher in F-MEN1 than in S-MEN1 (p = 0.009) and in MEN1 mutation-positive than in MEN1 mutation-negative (p = 0.01) index cases. In the whole cohort, the prevalence of lipomas was significantly higher in MEN1 mutation-positive compared to MEN1 mutation-negative patients (OR = 2.7, p = 0.02) and in F-MEN1 than in S-MEN1 (p = 0.03), only after adjustment for age. No significant differences were observed for the other non-endocrine manifestations between the two cohorts. Hibernoma and collagenoma were each present in one patient (0.5%) and meningioma and neuroblastoma in 2.7% and 0.5%, respectively. Gastric leiomyoma was present in 1.1% of the patients and uterine leiomyoma in 14% of women. Thyroid cancer, breast cancer, lung cancer, basal cell carcinoma, melanoma, and colorectal cancer were present in 4.9%, 2.7%, 1.6%, 1.6%, 2.2%, and 0.5% of the whole series, respectively.
Conclusions: We found a significantly higher prevalence of angiofibromas and lipomas in F-MEN1 compared with S-MEN1 and in MEN1 mutation-positive compared to MEN1 mutation-negative patients. In patients with one major endocrine manifestation of MEN1 , the presence of cutaneous lesions might suggest the diagnosis of MEN1 and a possible indication for genetic screening.
Keywords: GEP; adrenal; angiofibroma; cutaneous lesions; lipoma; pancreas; pituitary; primary hyperparathyroidism.
Copyright © 2023 Pierotti, Pardi, Dinoi, Piaggi, Borsari, Della Valentina, Sardella, Michelucci, Caligo, Bogazzi, Marcocci and Cetani.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Pardi E, Borsari S, Saponaro F, Bogazzi F, Urbani C, Mariotti S, et al. Mutational and large deletion study of genes implicated in hereditary forms of primary hyperparathyroidism and correlation with clinical features. PloS One (2017) 12(10):e0186485. doi: 10.1371/journal.pone.0186485 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources