

Respiratory infections predominate after day 100 following B-cell maturation antigen-directed CAR T-cell therapy
- PMID: 37486599
- PMCID: PMC10514400
- DOI: 10.1182/bloodadvances.2023010524
Respiratory infections predominate after day 100 following B-cell maturation antigen-directed CAR T-cell therapy
Abstract
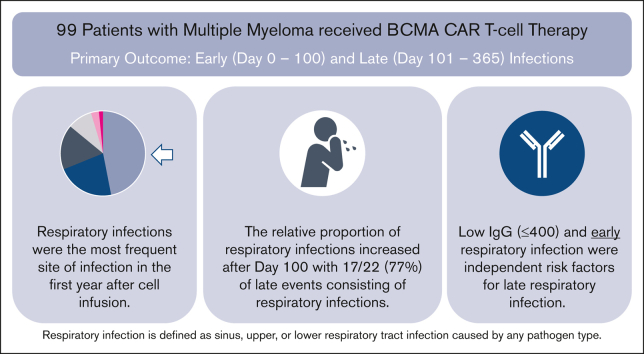
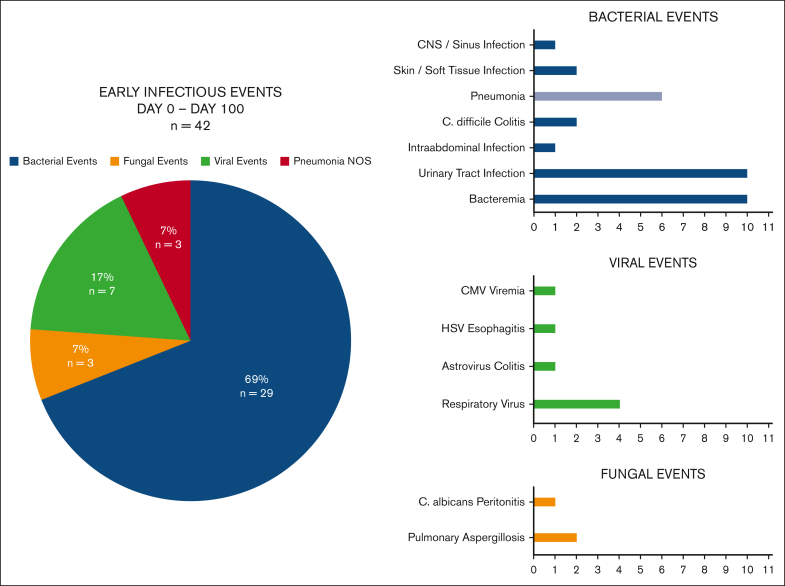
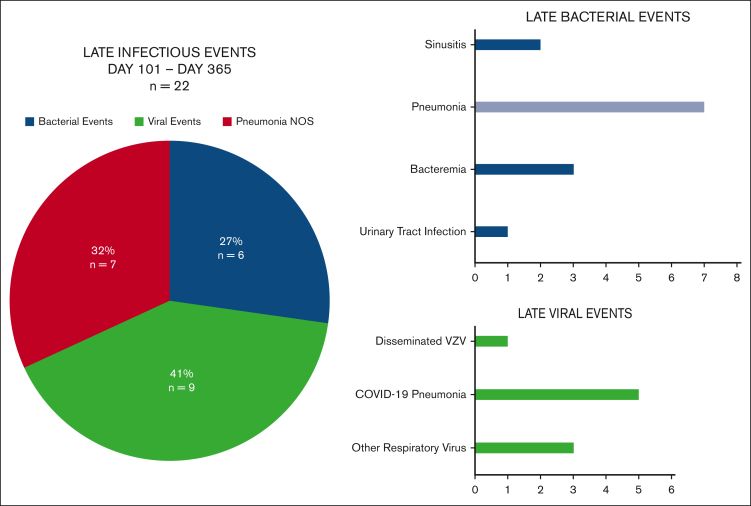
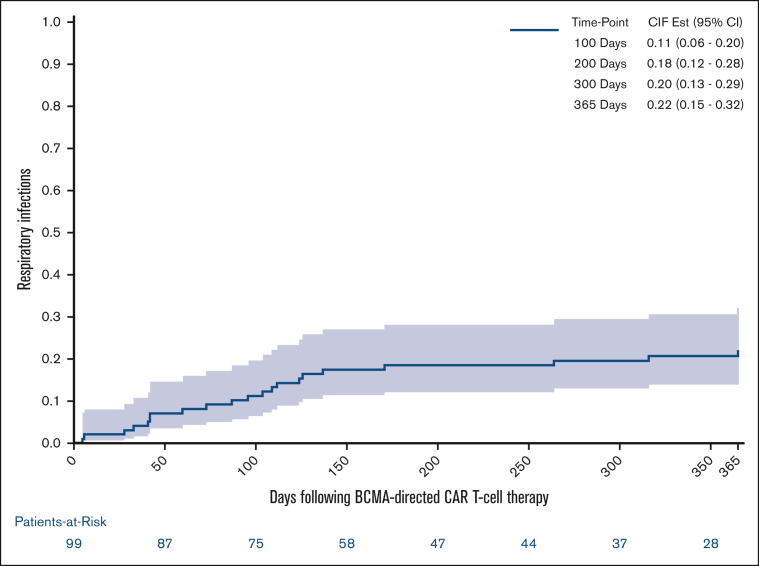
Infections are an important complication after B-cell maturation antigen (BCMA)-directed chimeric antigen receptor (CAR) T-cell therapy and risks may differ between the early and late periods. We evaluated infections in 99 adults who received a first BCMA-directed CAR T-cell therapy (commercial and investigational autologous BCMA CAR T-cell products at the recommended phase 2 dose) for relapsed/refractory multiple myeloma between November 2016 and May 2022. Infections were recorded until day 365, if patients experienced symptoms with a microbiologic diagnosis, or for symptomatic site-specific infections treated with antimicrobials. One-year cumulative incidence functions were calculated based on time to first respiratory infection using dates of infection-free death and receipt of additional antineoplastic therapies as competing risks. Secondary analysis evaluated risk factors for late respiratory infections using univariate and multivariable Cox regression models. Thirty-seven patients (37%) experienced 64 infectious events over the first year after BCMA-directed CAR T-cell therapy, with 42 early infectious events (days, 0-100), and 22 late infectious events (days, 101-365). Respiratory infections were the most common site-specific infection and the relative proportion of respiratory infections increased in the late period (31% of early events vs 77% of late events). On multivariable analysis, hypogammaglobulinemia (hazard ratio [HR], 6.06; P = .044) and diagnosis of an early respiratory viral infection (HR, 2.95; P = .048) were independent risk factors for late respiratory infection. Respiratory infections predominate after BCMA CAR T-cell therapy, particularly after day 100. Hypogammaglobulinemia and diagnosis of an early respiratory infection are risk factors for late respiratory infections that may be used to guide targeted preventive strategies.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: O.N. serves on advisory board of Janssen, BMS, Karyopharm, GPCR therapeutics, GSK, and Sanofi; and consults for GPCR therapeutics and Janssen. A.S. receives consulting fee from Novartis and Roche. N.R. receives consulting/advisory board membership fee from Pfizer, BMS, Janssen, Sanofi, AbbVie, Regeneron, Amgen, Caribou, and Immuneel; research funding from Pfizer and 2Seventybio. N.M. receives consulting fee from Takeda, Janssen, OncoPeptides, AbbVie, Adaptive, Amgen, BeiGene, Karyopharm Therapeutics, BMS, Celgene, Legend Biotech, Novartis, Sebia, Raqia, and Pfizer; has stock/patents/royalties in OncoPeptides, C4 therapuetics, and Raquia; is on the board of directors of OncoPeptides; and is the President of the International Myeloma Society. M.F. receives consulting fee from Celgene, Novartis, Kite, and Iovance. S.P.H. receives consulting from Pfizer. The remaining authors declare no competing financial interests.
Figures
References
-
- Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839–852. - PubMed
-
- Munshi NC, Anderson LD, Jr., Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
