

Pitavastatin to Prevent Cardiovascular Disease in HIV Infection
- PMID: 37486775
- PMCID: PMC10564556
- DOI: 10.1056/NEJMoa2304146
Pitavastatin to Prevent Cardiovascular Disease in HIV Infection
Update in
-
Trial Update of Pitavastatin to Prevent Cardiovascular Events in HIV Infection.N Engl J Med. 2024 May 2;390(17):1626-1628. doi: 10.1056/NEJMc2400870. N Engl J Med. 2024. PMID: 38692296 Free PMC article. No abstract available.
Abstract
Background: The risk of cardiovascular disease is increased among persons with human immunodeficiency virus (HIV) infection, so data regarding primary prevention strategies in this population are needed.
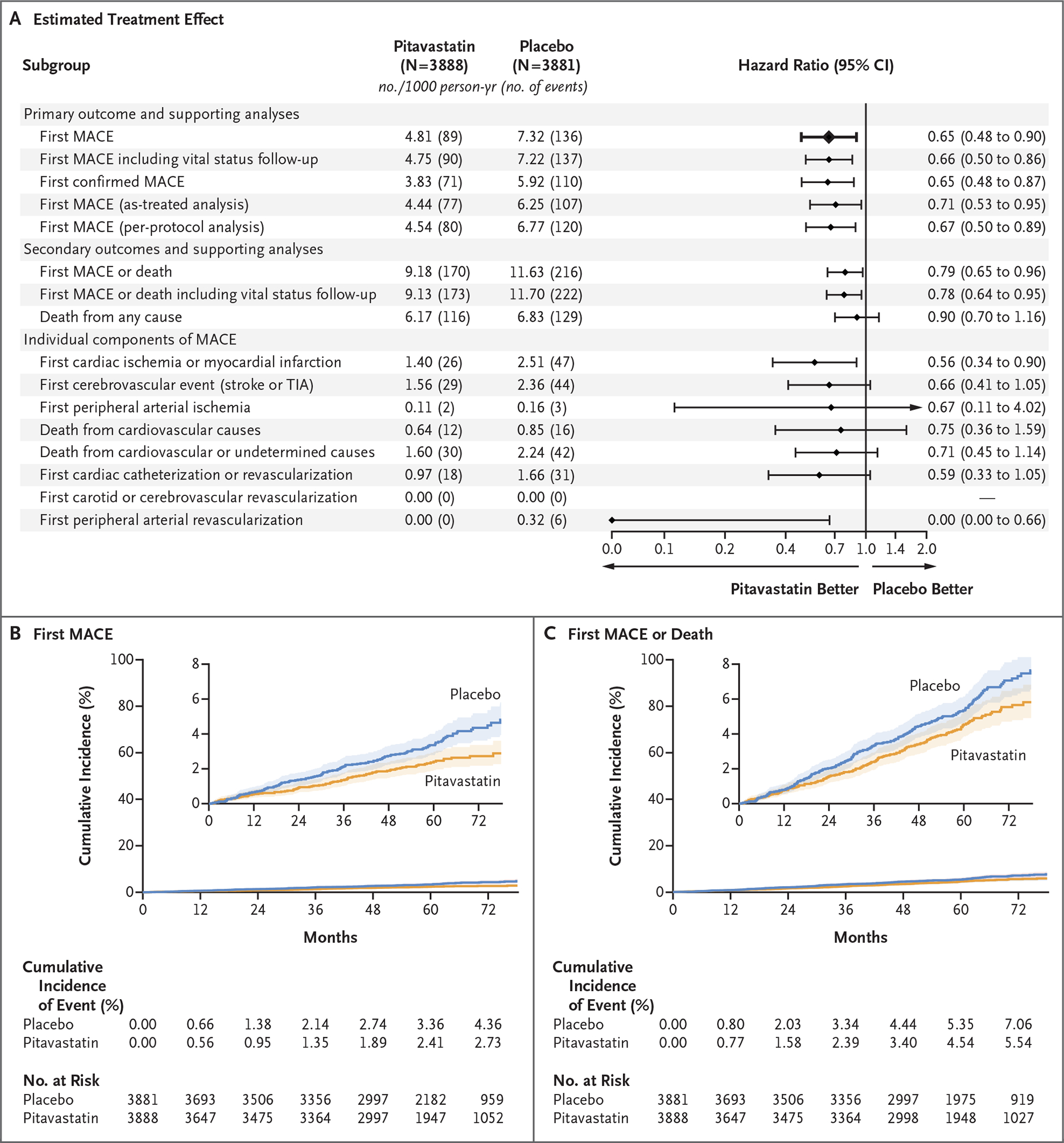
Methods: In this phase 3 trial, we randomly assigned 7769 participants with HIV infection with a low-to-moderate risk of cardiovascular disease who were receiving antiretroviral therapy to receive daily pitavastatin calcium (at a dose of 4 mg) or placebo. The primary outcome was the occurrence of a major adverse cardiovascular event, which was defined as a composite of cardiovascular death, myocardial infarction, hospitalization for unstable angina, stroke, transient ischemic attack, peripheral arterial ischemia, revascularization, or death from an undetermined cause.
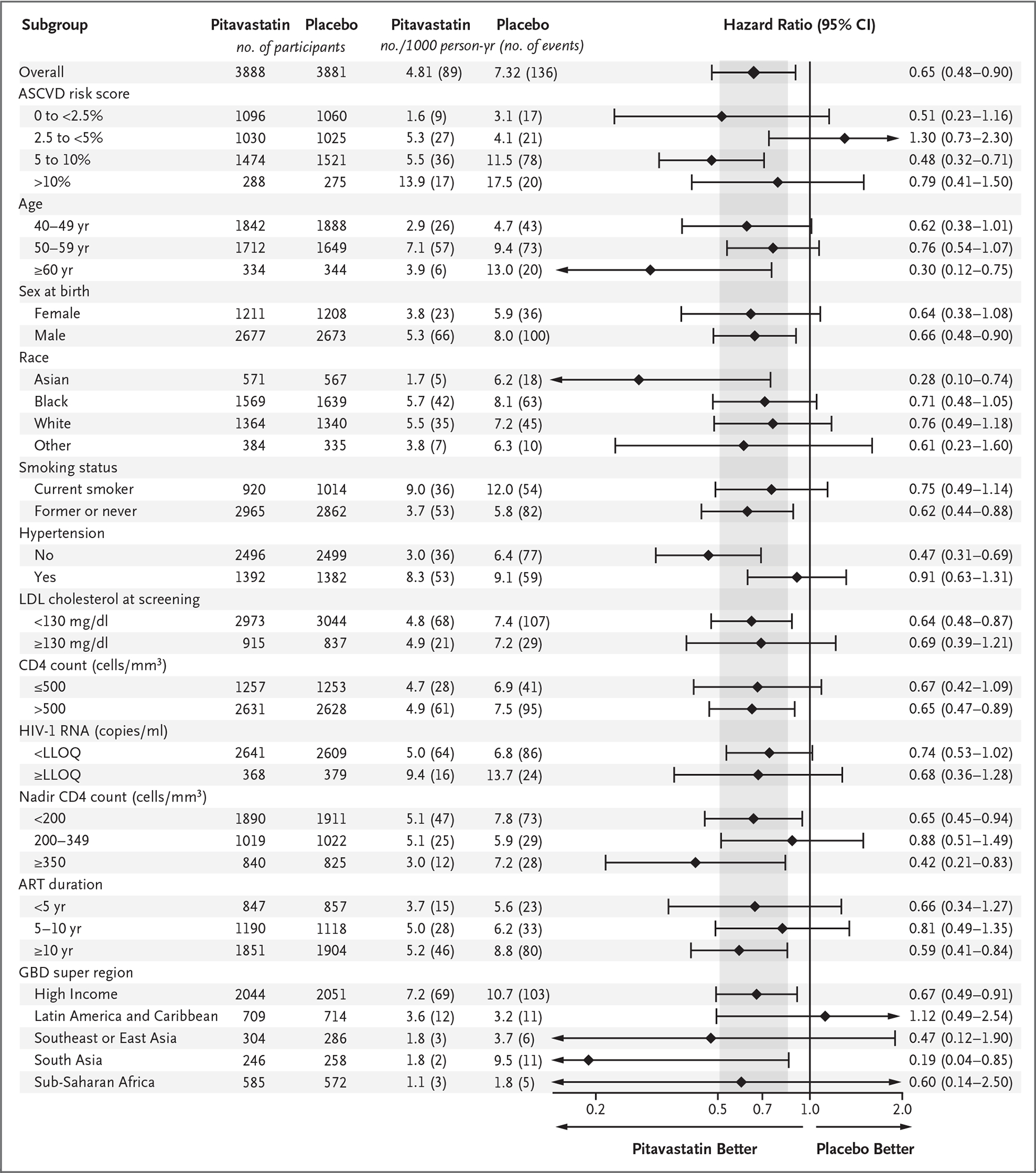
Results: The median age of the participants was 50 years (interquartile range, 45 to 55); the median CD4 count was 621 cells per cubic millimeter (interquartile range, 448 to 827), and the HIV RNA value was below quantification in 5250 of 5997 participants (87.5%) with available data. The trial was stopped early for efficacy after a median follow-up of 5.1 years (interquartile range, 4.3 to 5.9). The incidence of a major adverse cardiovascular event was 4.81 per 1000 person-years in the pitavastatin group and 7.32 per 1000 person-years in the placebo group (hazard ratio, 0.65; 95% confidence interval [CI], 0.48 to 0.90; P = 0.002). Muscle-related symptoms occurred in 91 participants (2.3%) in the pitavastatin group and in 53 (1.4%) in the placebo group; diabetes mellitus occurred in 206 participants (5.3%) and in 155 (4.0%), respectively.
Conclusions: Participants with HIV infection who received pitavastatin had a lower risk of a major adverse cardiovascular event than those who received placebo over a median follow-up of 5.1 years. (Funded by the National Institutes of Health and others; REPRIEVE ClinicalTrials.gov number, NCT02344290.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Pitavastatin reduces cardiovascular events in patients with HIV infection.Nat Rev Cardiol. 2023 Oct;20(10):648. doi: 10.1038/s41569-023-00920-z. Nat Rev Cardiol. 2023. PMID: 37587223 No abstract available.
-
Cardiovascular disease prevention in people living with HIV: from REPRIEVE to a statin of grace.Eur Heart J. 2023 Nov 1;44(41):4308-4309. doi: 10.1093/eurheartj/ehad594. Eur Heart J. 2023. PMID: 37674466 No abstract available.
-
In adults with HIV and low-to-moderate CV risk, pitavastatin reduced MACE over a median 5.1 y.Ann Intern Med. 2023 Nov;176(11):JC130. doi: 10.7326/J23-0083. Epub 2023 Nov 7. Ann Intern Med. 2023. PMID: 37931263
-
Pitavastatin and Cardiovascular Disease in HIV.N Engl J Med. 2023 Nov 23;389(21):e46. doi: 10.1056/NEJMc2311117. N Engl J Med. 2023. PMID: 37991864 No abstract available.
-
Pitavastatin and Cardiovascular Disease in HIV.N Engl J Med. 2023 Nov 23;389(21):e46. doi: 10.1056/NEJMc2311117. N Engl J Med. 2023. PMID: 37991865 No abstract available.
-
Pitavastatin and Cardiovascular Disease in HIV.N Engl J Med. 2023 Nov 23;389(21):e46. doi: 10.1056/NEJMc2311117. N Engl J Med. 2023. PMID: 37991866 No abstract available.
-
Pitavastatin and Cardiovascular Disease in HIV.N Engl J Med. 2023 Nov 23;389(21):e46. doi: 10.1056/NEJMc2311117. N Engl J Med. 2023. PMID: 37991867 No abstract available.
-
Pitavastatin and Cardiovascular Disease in HIV. Reply.N Engl J Med. 2023 Nov 23;389(21):e46. doi: 10.1056/NEJMc2311117. N Engl J Med. 2023. PMID: 37991868 No abstract available.
References
-
- Zanni MV, Schouten J, Grinspoon SK, Reiss P. Risk of coronary heart disease in patients with HIV infection. Nat Rev Cardiol 2014;11:728–41. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069456/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- U01HL123339/HL/NHLBI NIH HHS/United States
- I01 BX000207/BX/BLRD VA/United States
- U01HL123336/HL/NHLBI NIH HHS/United States
- K24 AI157882/AI/NIAID NIH HHS/United States
- UM1 AI069463/AI/NIAID NIH HHS/United States
- U01 AI069424/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- UG3 HL164285/HL/NHLBI NIH HHS/United States
- P30 DK040561/DK/NIDDK NIH HHS/United States
- UM1 AI069470/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 HL123339/HL/NHLBI NIH HHS/United States
- UM1 AI069496/AI/NIAID NIH HHS/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- U01 HL123336/HL/NHLBI NIH HHS/United States
- U24 HL164284/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials