

Experimental evidence for structured information-sharing networks reducing medical errors
- PMID: 37487106
- PMCID: PMC10401006
- DOI: 10.1073/pnas.2108290120
Experimental evidence for structured information-sharing networks reducing medical errors
Abstract
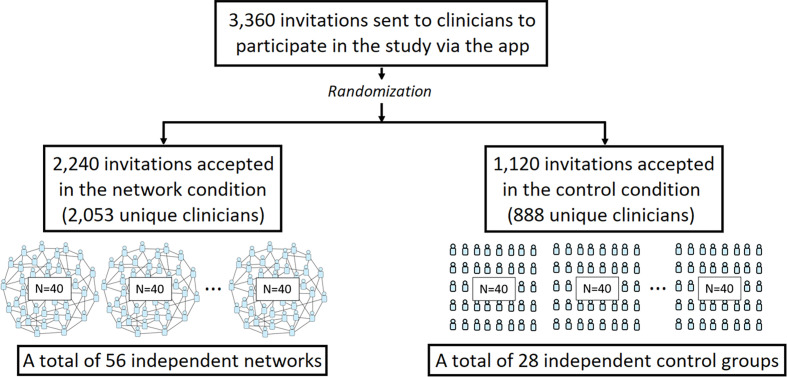
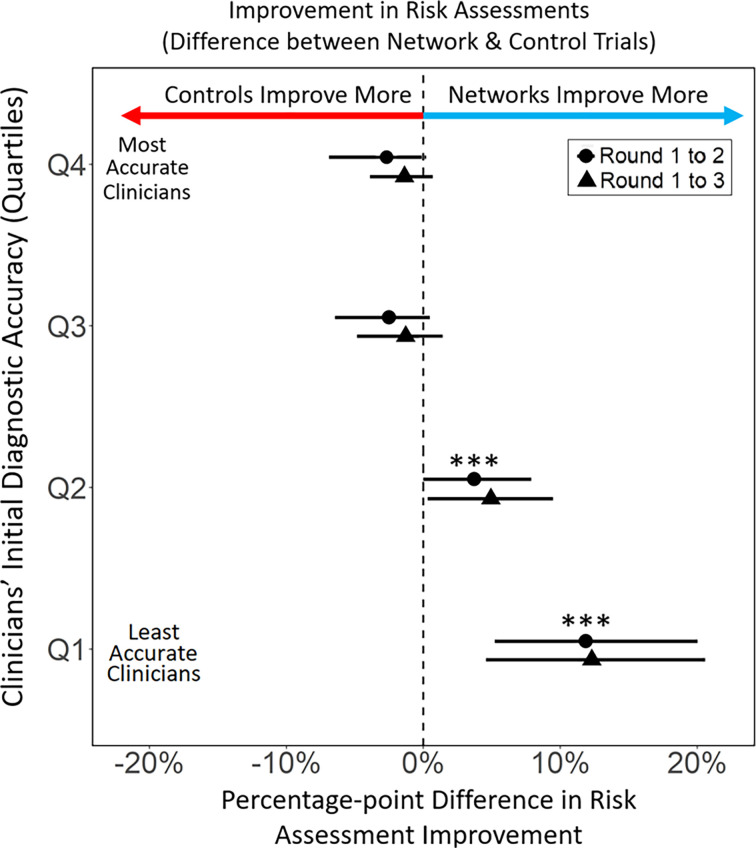
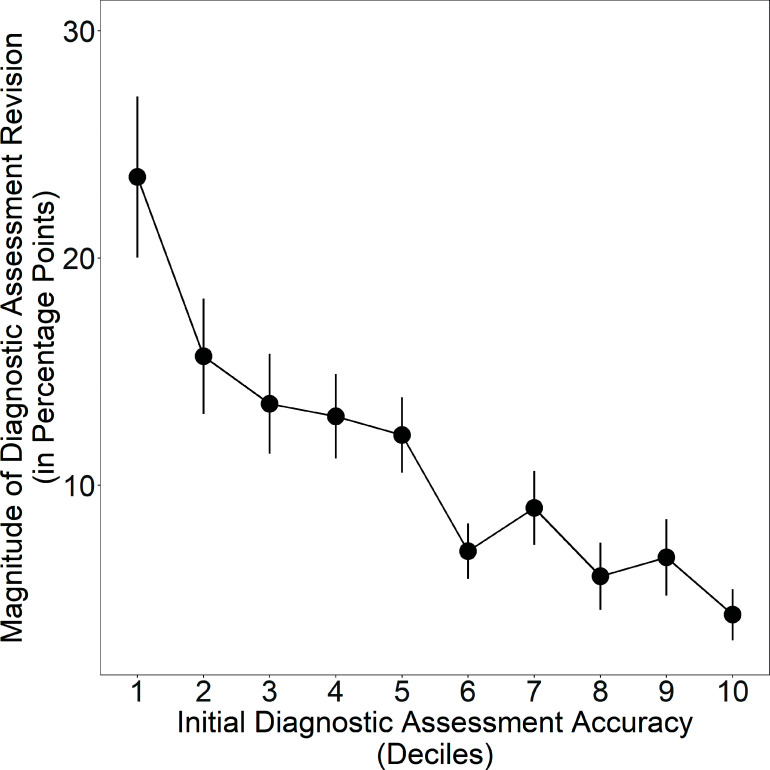
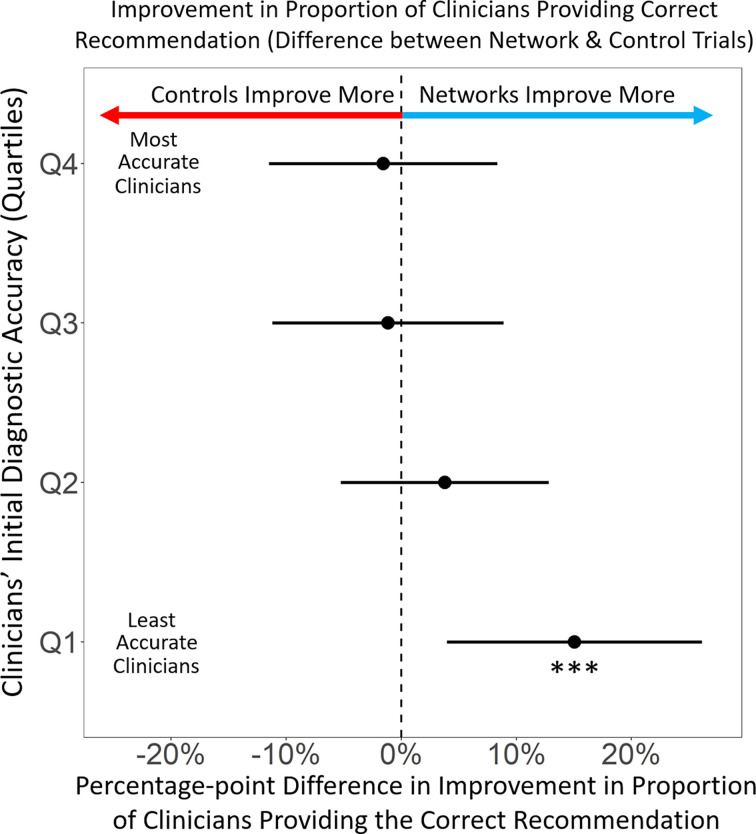
Errors in clinical decision-making are disturbingly common. Recent studies have found that 10 to 15% of all clinical decisions regarding diagnoses and treatment are inaccurate. Here, we experimentally study the ability of structured information-sharing networks among clinicians to improve clinicians' diagnostic accuracy and treatment decisions. We use a pool of 2,941 practicing clinicians recruited from around the United States to conduct 84 independent group-level trials, ranging across seven different clinical vignettes for topics known to exhibit high rates of diagnostic or treatment error (e.g., acute cardiac events, geriatric care, low back pain, and diabetes-related cardiovascular illness prevention). We compare collective performance in structured information-sharing networks to collective performance in independent control groups, and find that networks significantly reduce clinical errors, and improve treatment recommendations, as compared to control groups of independent clinicians engaged in isolated reflection. Our results show that these improvements are not a result of simple regression to the group mean. Instead, we find that within structured information-sharing networks, the worst clinicians improved significantly while the best clinicians did not decrease in quality. These findings offer implications for the use of social network technologies to reduce errors among clinicians.
Keywords: collective intelligence; decision-making; medical errors; networks.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Leape L. L., et al. , The nature of adverse events in hospitalized patients: Results of the harvard medical practice study II. N. Engl. J. Med. 324, 377–384 (1991). - PubMed
-
- Wachter R. M., Why diagnostic errors don’t get any respect—And what can be done about them. Health Affairs 29, 1605–1610 (2010). - PubMed
-
- “Committee on diagnostic error in health care, Board on health care services, Institute of medicine, The national academies of sciences, engineering, and medicine, improving diagnosis” in Health Care, Balogh E. P., Miller B. T., Ball J. R., Eds. (National Academies Press, US, 2015) (January 5, 2023).
-
- Kattan M. W., O’Rourke C., Yu C., Chagin K., The wisdom of crowds of doctors: Their average predictions outperform their individual ones. Med. Decis. Making 36, 536–540 (2016). - PubMed
