

Molecular Tumor Board as a Clinical Tool for Converting Molecular Data Into Real-World Patient Care
- PMID: 37487147
- PMCID: PMC10581623
- DOI: 10.1200/PO.23.00067
Molecular Tumor Board as a Clinical Tool for Converting Molecular Data Into Real-World Patient Care
Abstract
Purpose: The investigation of multiple molecular targets with next-generation sequencing (NGS) has entered clinical practice in oncology, yielding to a paradigm shift from the histology-centric approach to the mutational model for personalized treatment. Accordingly, most of the drugs recently approved in oncology are coupled to specific biomarkers. One potential tool for implementing the mutational model of precision oncology in daily practice is represented by the Molecular Tumor Board (MTB), a multidisciplinary team whereby molecular pathologists, biologists, bioinformaticians, geneticists, medical oncologists, and pharmacists cooperate to generate, interpret, and match molecular data with personalized treatments.
Patients and methods: Since May 2020, the institutional MTB set at Fondazione IRCCS Istituto Nazionale Tumori of Milan met weekly via teleconference to discuss molecular data and potential therapeutic options for patients with advanced/metastatic solid tumors.
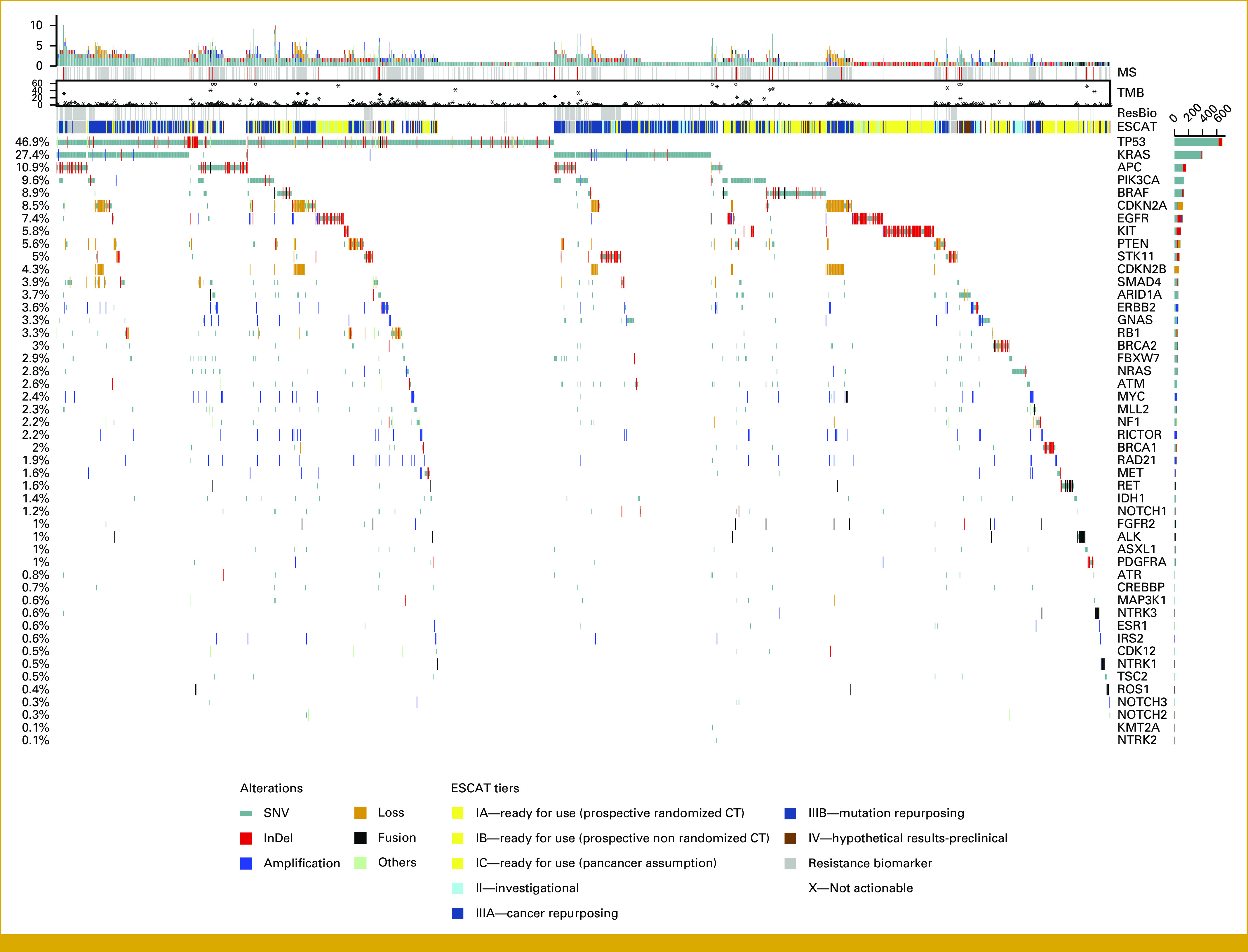
Results: Up to October 2021, among 1,996 patients evaluated, we identified >10,000 variants, 43.2% of which were functionally relevant (pathogenic or likely pathogenic). On the basis of functionally relevant variants, 711 patients (35.6%) were potentially eligible to targeted therapy according to European Society of Medical Oncology Scale for Clinical Actionability of Molecular Targets tiers, and 9.4% received a personalized treatment. Overall, larger NGS panels (containing >50 genes) significantly outperformed small panels (up to 50 genes) in detecting actionable gene targets across different tumor types.
Conclusion: Our real-world data provide evidence that MTB is a valuable tool for matching NGS data with targeted treatments, eventually implementing precision oncology in clinical practice.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures




References
-
- Bedard PL, Hyman DM, Davids MS, et al. Small molecules, big impact: 20 years of targeted therapy in oncology. Lancet. 2020;395:1078–1088. - PubMed
-
- 2021. https://www.iqvia.com/insights/the-iqvia-institute/reports/global-oncolo... IQVIA Global Oncology Trends 2021.
-
- 2021. https://www.ema.europa.eu/en/annual-report/2021/index.html EMA annual report 2021.
-
- Mosele F, Remon J, Mateo J, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO Precision Medicine Working Group. Ann Oncol. 2020;31:1491–1505. - PubMed
-
- Filetti S, Durante C, Hartl DM, et al. ESMO Clinical Practice Guideline update on the use of systemic therapy in advanced thyroid cancer. Ann Oncol. 2022;33:674–684. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
