

doi: 10.1503/cmaj.221510-f.
Myopéricardite persistante après une vaccination hétérologue à ARNm anti-SRAS-CoV-2
[Article in
French]
Affiliations
- PMID: 37487616
- PMCID: PMC10365856
- DOI: 10.1503/cmaj.221510-f
Item in Clipboard
Myopéricardite persistante après une vaccination hétérologue à ARNm anti-SRAS-CoV-2
[Article in
French]
CMAJ.
.
No abstract available
Conflict of interest statement
Intérêts concurrents: Ian Paterson déclare avoir reçu des honoraires de conférencier des sociétés Pfizer Canada et AstraZeneca. Aucun autre intérêt concurrent n’a été déclaré.
Figures
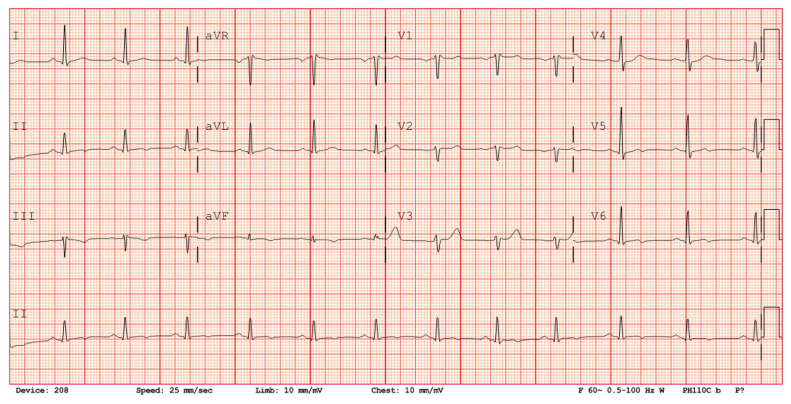
Électrocardiogramme d’un homme de 41 ans à son arrivée à notre hôpital; on voit un rythme sinusal et des anomalies de l’onde T inféroapicales non spécifiques sans déviation du segment ST.
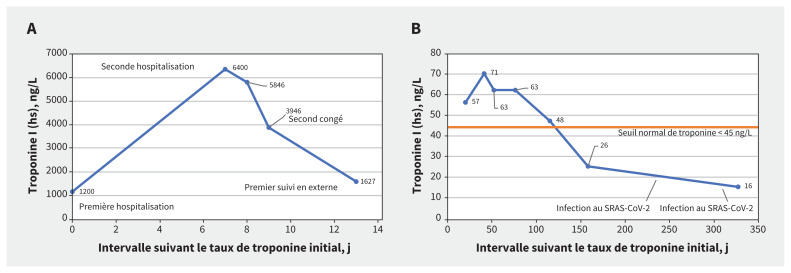
Tendance temporelle des taux de troponine I de haute sensibilité (hs) aux semaines (A) 1 et 2 (congé au jour 13) et (B) 3–45 suivant la première hospitalisation.
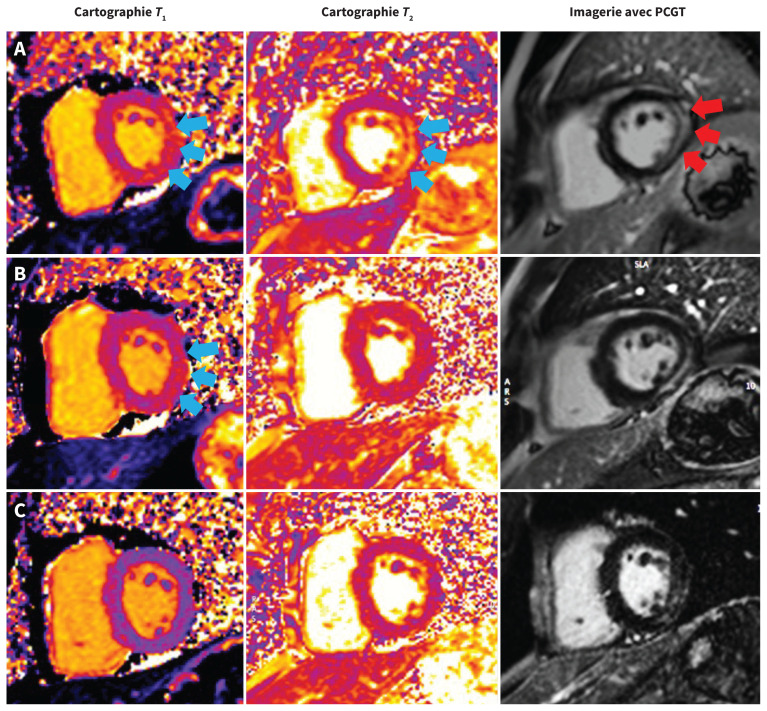
Imagerie par résonance magnétique cardiaque chez un homme de 41 ans atteint de myocardite. (A) Clichés de l’axe court oblique montrant un œdème de la paroi inférolatérale en T1 et T2 (flèches bleues) (T1 = 1083 ms [plage normale 950–1050 ms] et T2 = 71 ms [normale < 57 ms]) et à l’imagerie avec prise tardive de l’agent de contraste gadolinium (PCGT) (flèches rouges) durant l’hospitalisation. (B) Œdème myocardique persistant à la paroi inférolatérale en T1 (flèches bleues), mais non en T2 après 2 mois (T1 = 1080 ms; T2 = 48 ms). (C) Œdème myocardique résolu en T1 et en T2 après 6 mois (T1 = 1010 ms; T2 = 46 ms). Tous les clichés ont été acquis au moyen du même appareil d’IRM 1.5 T (Aera, Siemens Healthineers).
References
-
- Lurz P, Luecke C, Eitel I, et al. . Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-trial. J Am Coll Cardiol 2016;67:1800–11. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical