

Comparative Efficacy of Pharmacological Treatments for Acne Vulgaris: A Network Meta-Analysis of 221 Randomized Controlled Trials
- PMID: 37487721
- PMCID: PMC10365865
- DOI: 10.1370/afm.2995
Comparative Efficacy of Pharmacological Treatments for Acne Vulgaris: A Network Meta-Analysis of 221 Randomized Controlled Trials
Abstract
Purpose: Acne is an extremely common skin disease with an estimated global prevalence of 9.4%. We aim to provide comprehensive comparisons of the common pharmacological treatments for acne.
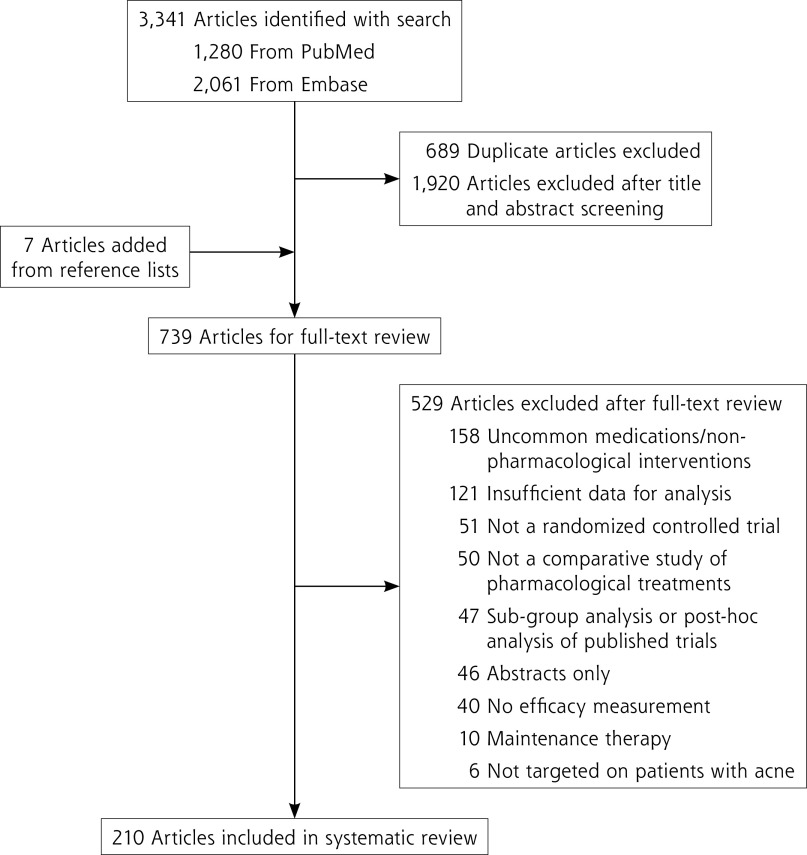
Methods: Randomized controlled trials comparing the efficacy of pharmacological therapies for acne vulgaris in patients of any age and sex and with a treatment duration of >2 weeks were included. PubMed and Embase databases were searched from inception until February 2022. Our prespecified primary end points were mean percentage reduction in total, inflammatory, and noninflammatory lesions. Treatment ranking was determined by P values.
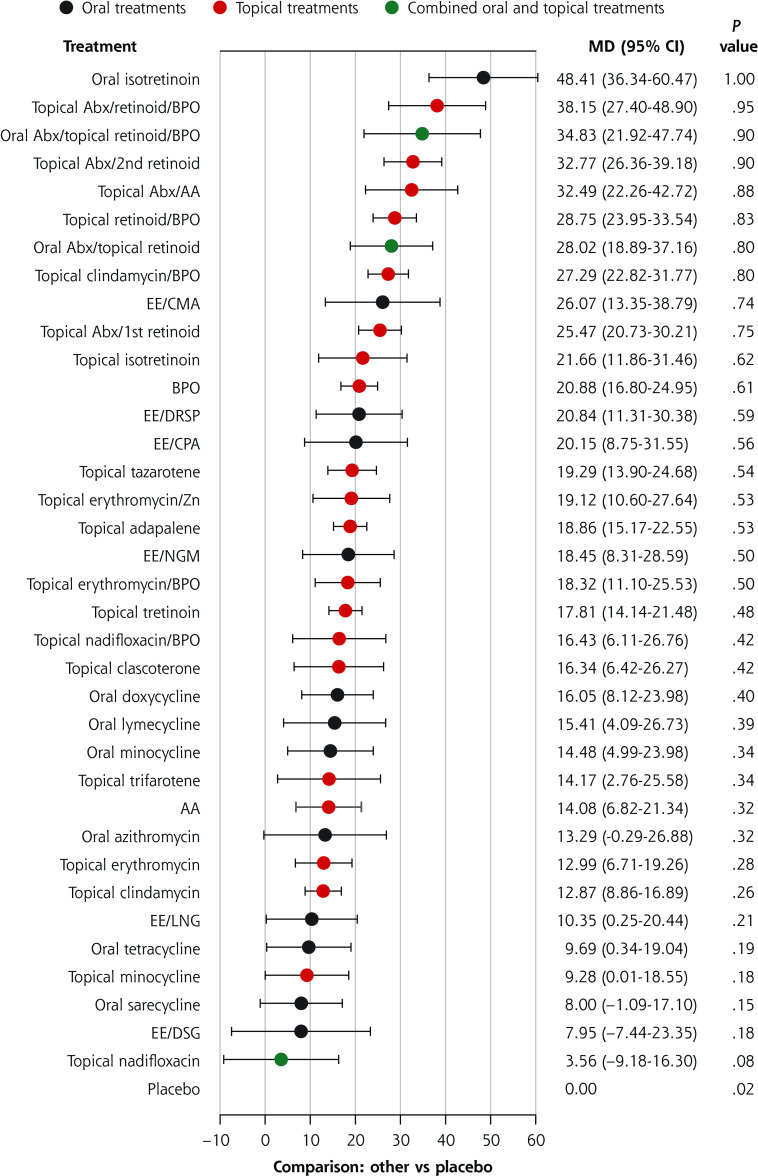
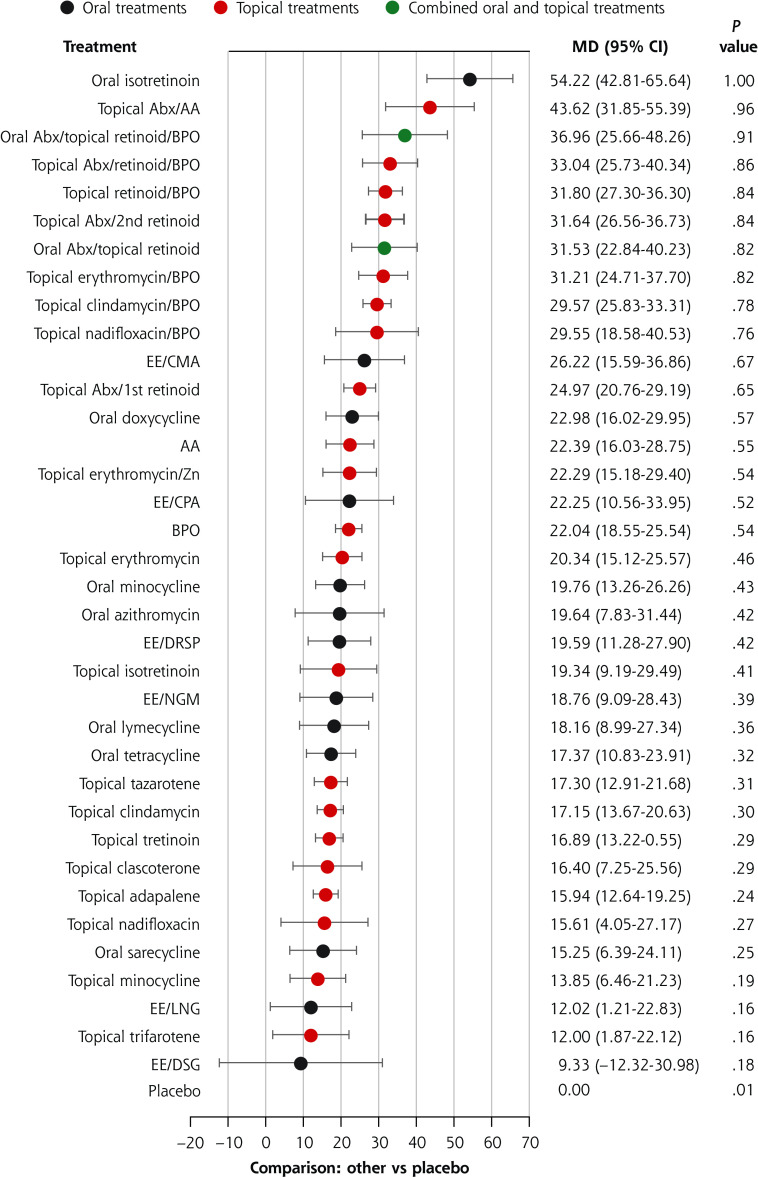
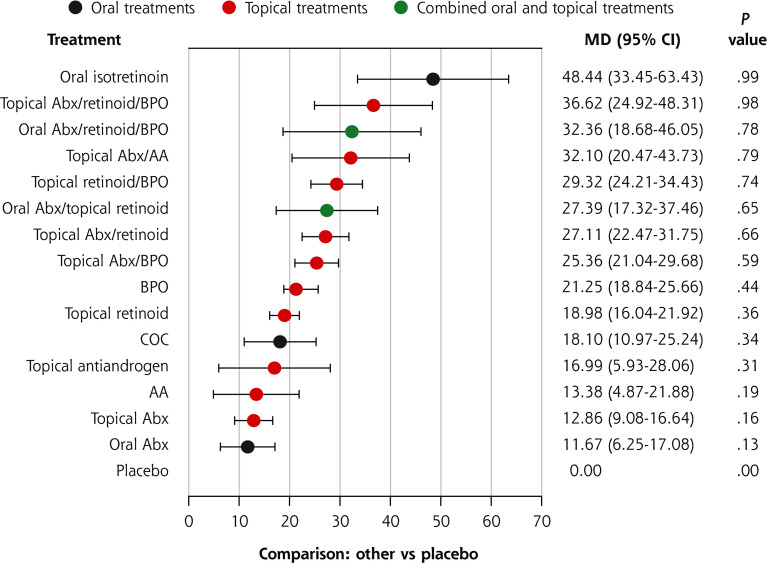
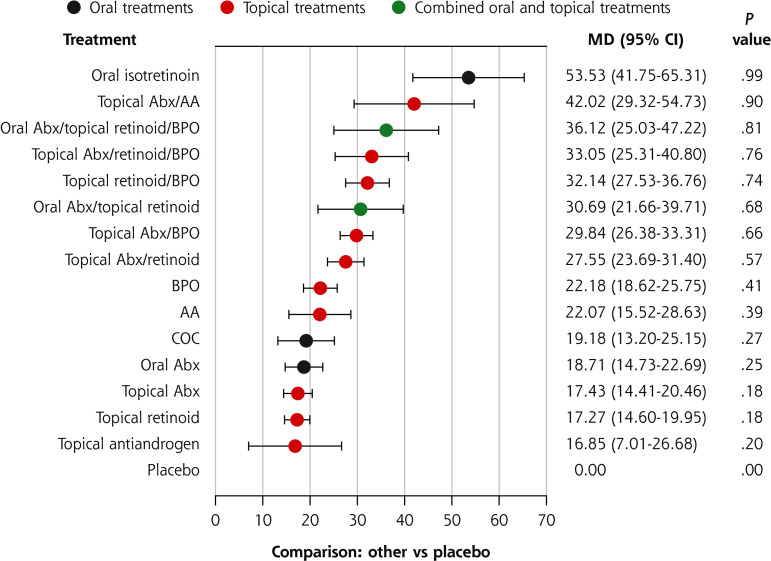
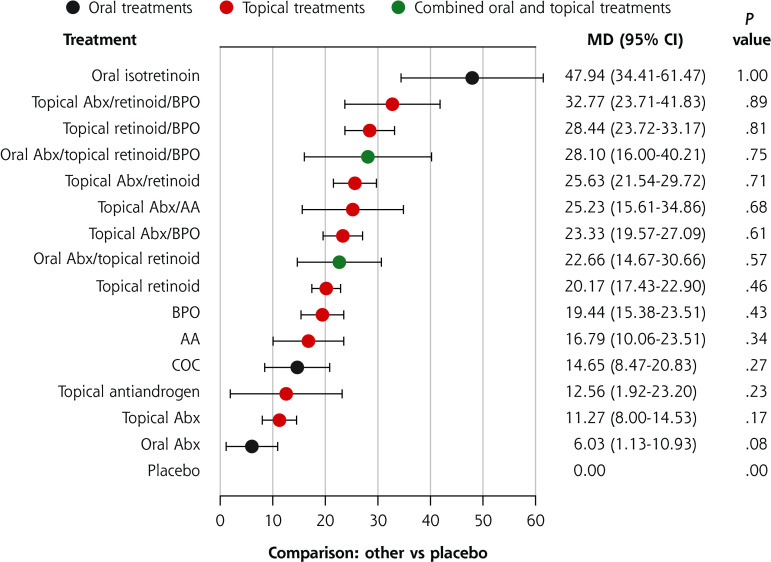
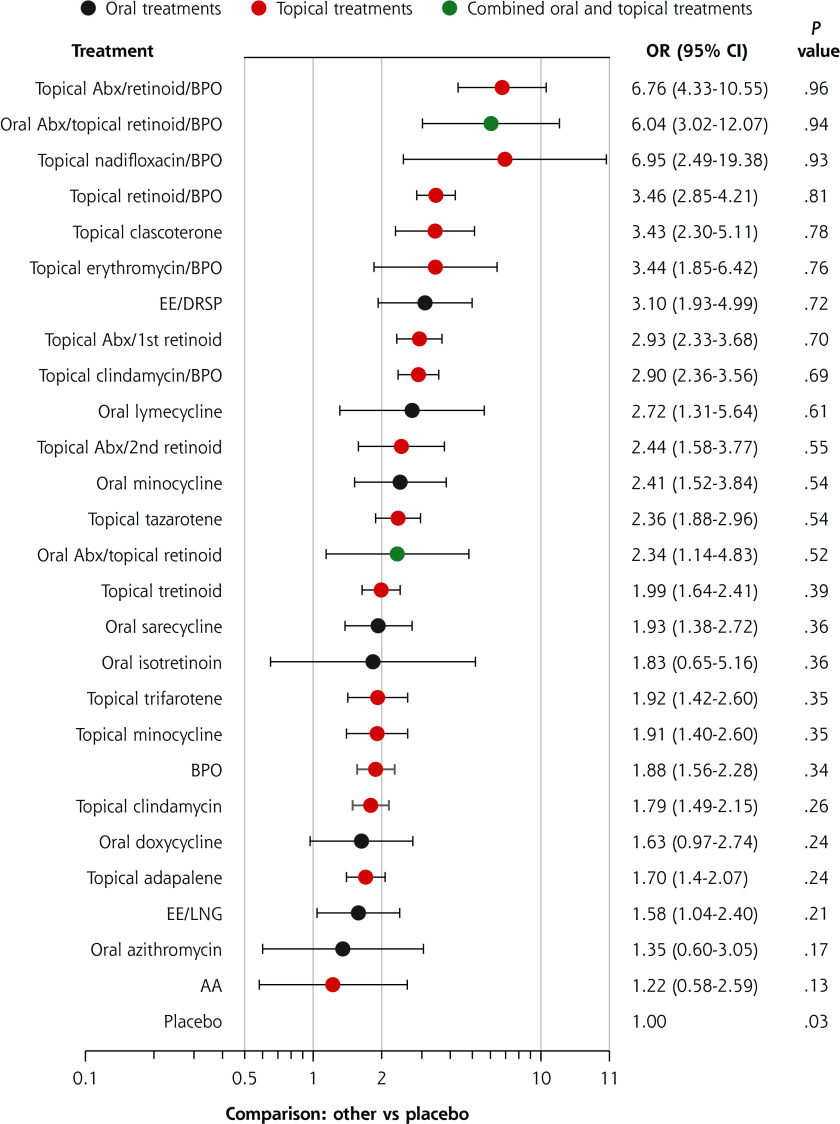
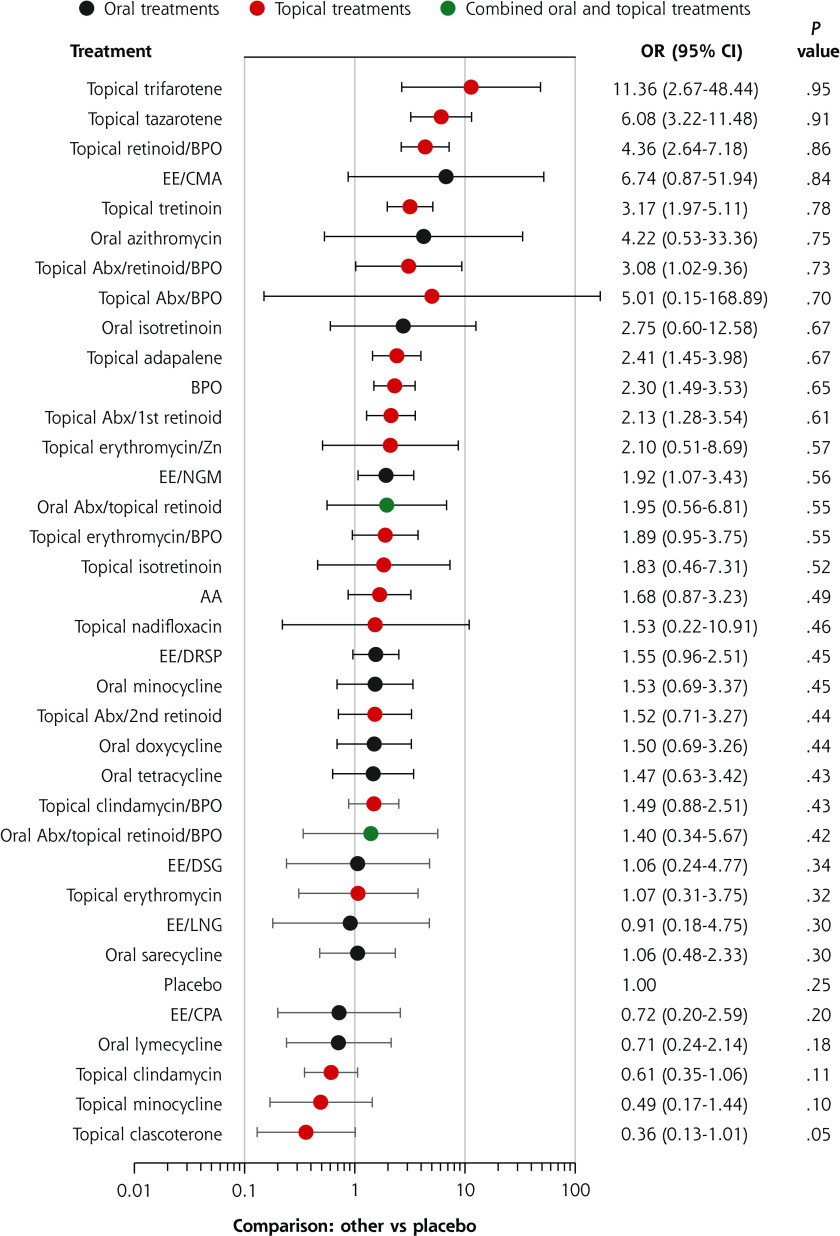
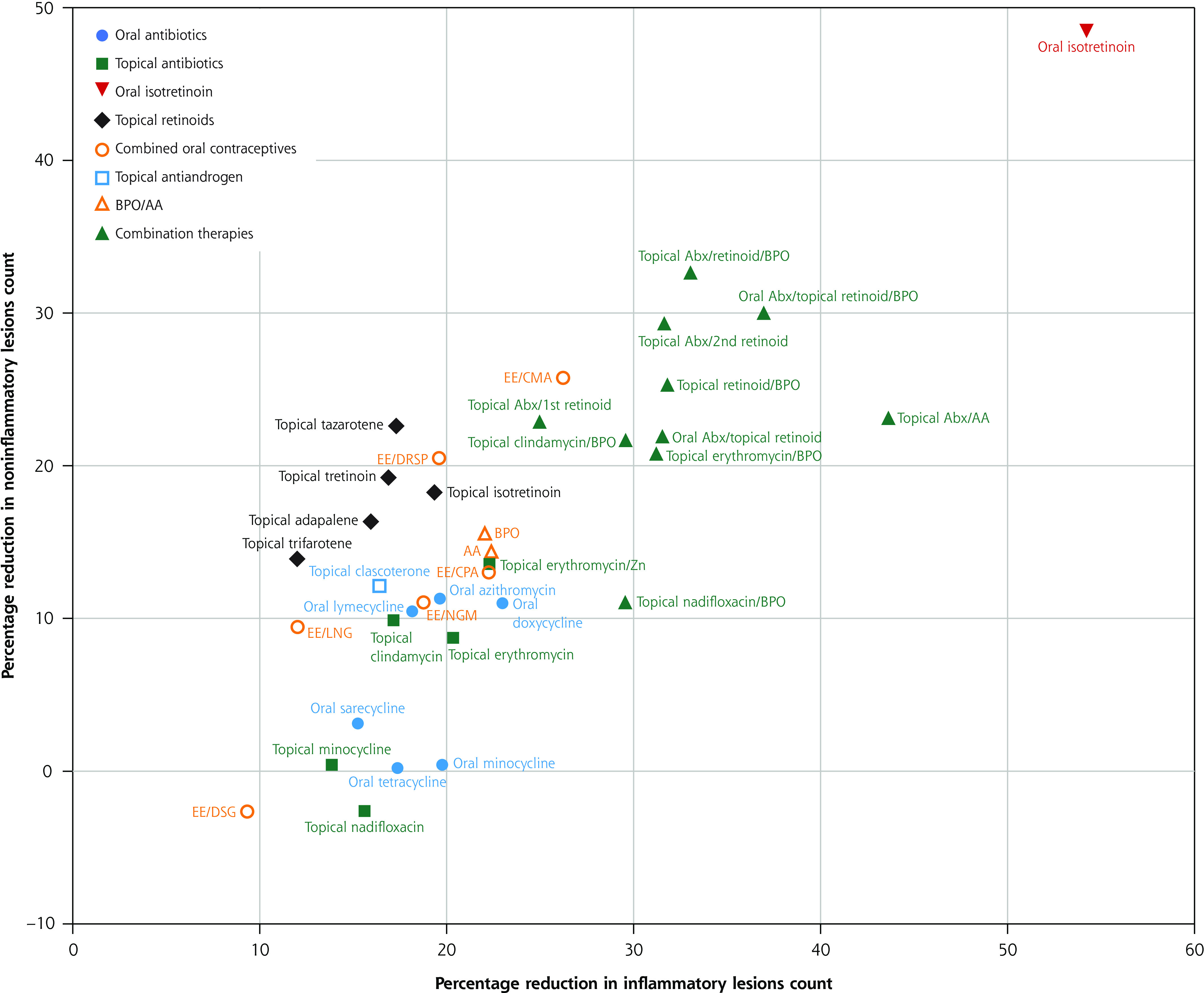
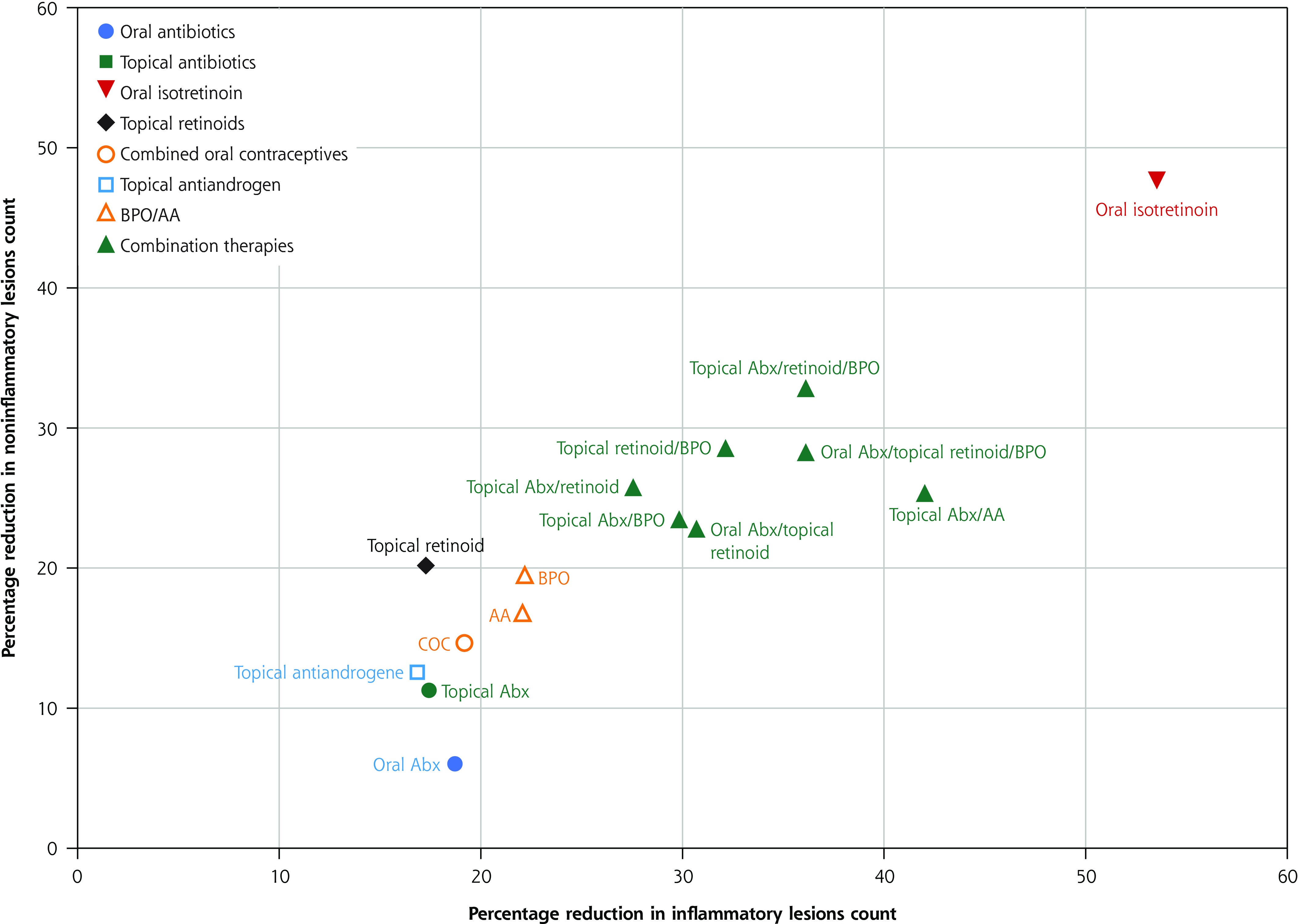
Results: There were 210 articles describing 221 trials and 37 interventions included in the analysis. Our primary analysis of percentage reduction in total lesion count had 65,601 patients enrolled. Across all trials, the mean age was 20.4 years. The median duration of treatment was 12 weeks. The median total, inflammatory, and noninflammatory lesion counts were 72, 27, and 44, respectively. The most effective treatment was oral isotretinoin (mean difference [MD] = 48.41; P = 1.00), followed by triple therapy containing a topical antibiotic, a topical retinoid, and benzoyl peroxide (BPO) (MD = 38.15; P = .95) and by triple therapy containing an oral antibiotic, a topical retinoid, and BPO (MD = 34.83; P = .90). For monotherapies, oral or topical antibiotics or topical retinoids have comparable efficacy for inflammatory lesions, while oral or topical antibiotics have less effect on noninflammatory lesions.
Conclusion: The most effective treatment for acne is oral isotretinoin, followed by triple therapies containing a topical retinoid, BPO, and an antibiotic. We present detailed comparisons of each intervention to serve as a practical database.
Keywords: acne vulgaris; anti-bacterial agents; drug therapy; network meta-analysis; retinoids.
© 2023 Annals of Family Medicine, Inc.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical