

A TLR7/8 agonist increases efficacy of anti-fentanyl vaccines in rodent and porcine models
- PMID: 37488109
- PMCID: PMC10366150
- DOI: 10.1038/s41541-023-00697-9
A TLR7/8 agonist increases efficacy of anti-fentanyl vaccines in rodent and porcine models
Abstract
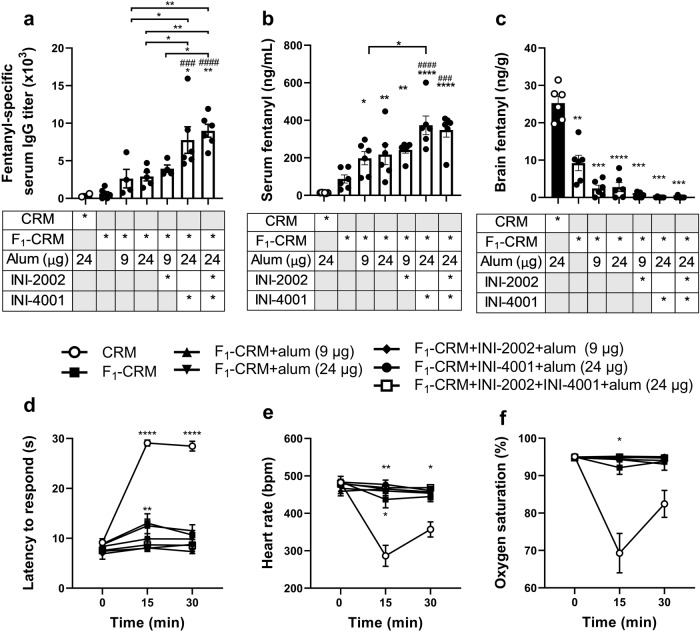
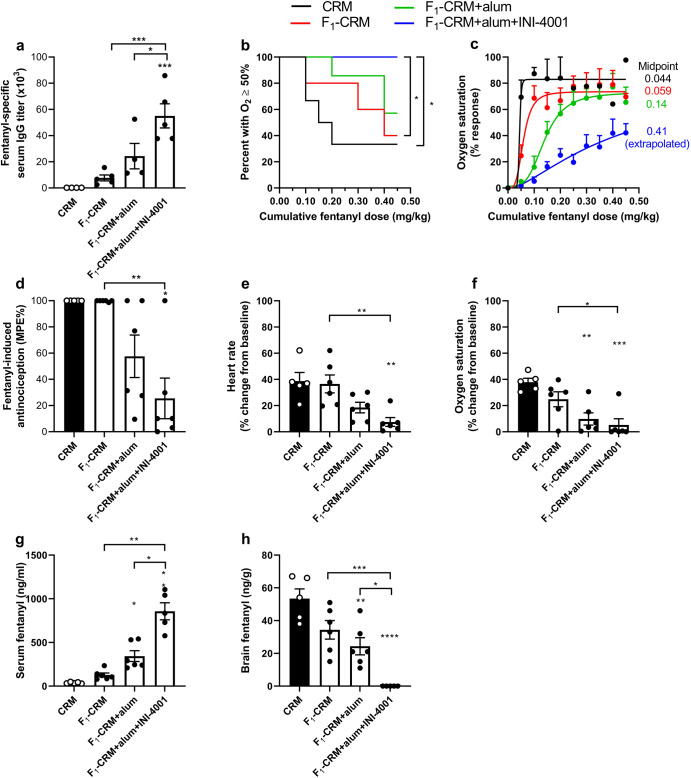
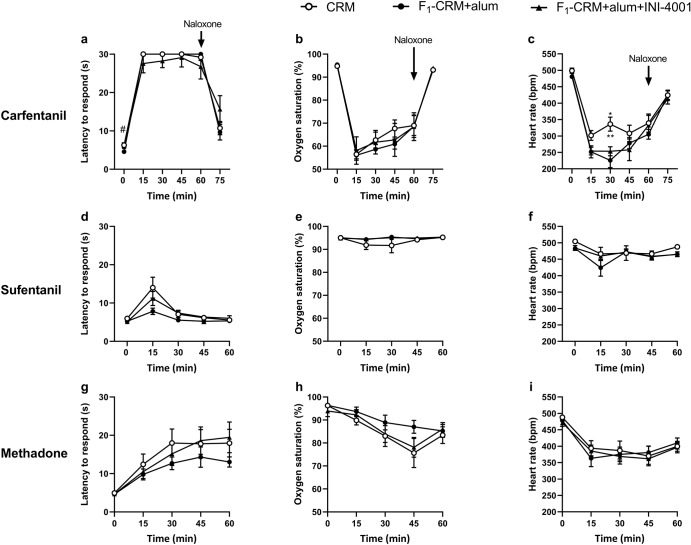
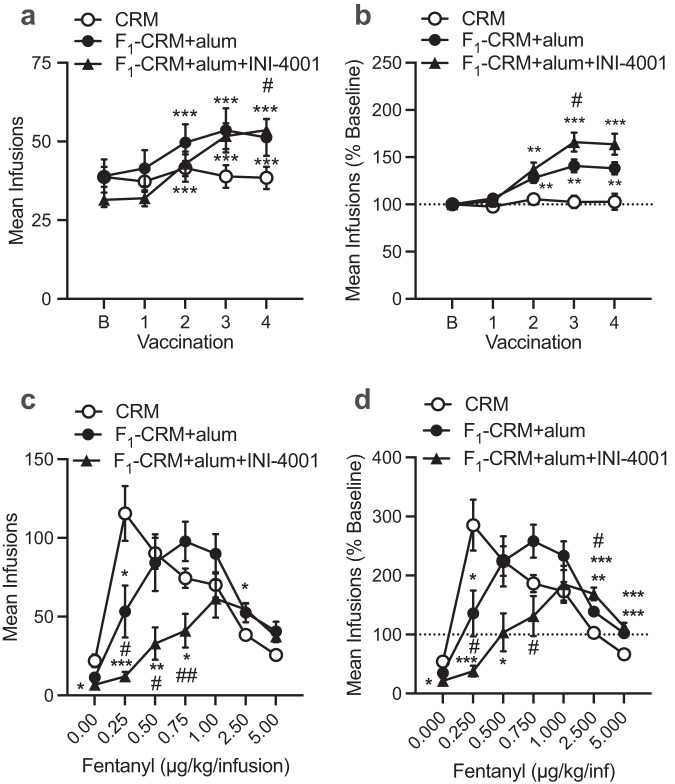
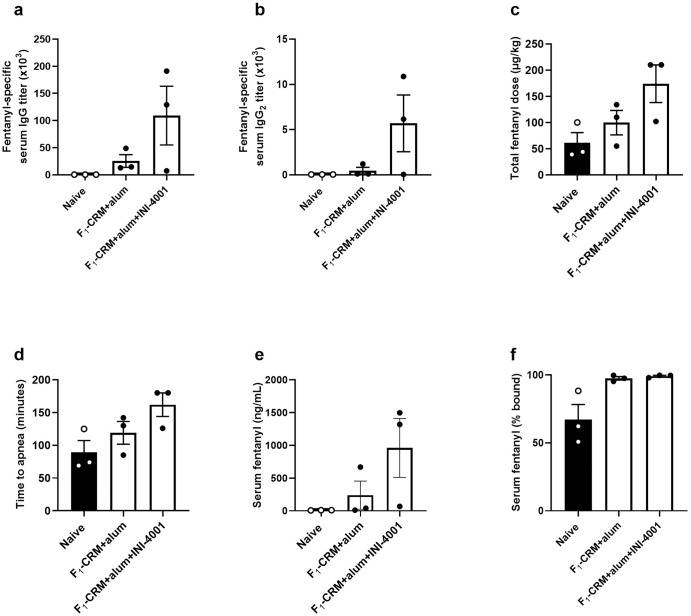
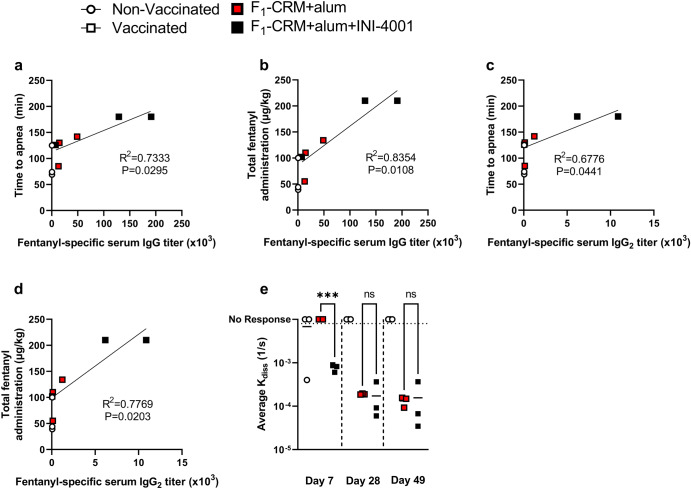
Opioid use disorders (OUD) and overdose are public health threats worldwide. Widespread access to highly potent illicit synthetic opioids such as fentanyl is driving the recent rise in fatal overdoses. Vaccines containing fentanyl-based haptens conjugated to immunogenic carrier proteins offer a long-lasting, safe, and cost-effective strategy to protect individuals from overdose upon accidental or deliberate exposure to fentanyl and its analogs. Prophylactic or therapeutic active immunization with an anti-fentanyl vaccine induces the production of fentanyl-specific antibodies that bind the drug in the blood and prevent its distribution to the brain, which reduces its reinforcing effects and attenuates respiratory depression and bradycardia. To increase the efficacy of a lead anti-fentanyl vaccine, this study tested whether the incorporation of synthetic toll-like receptor (TLR) 4 and TLR7/8 agonists as vaccine adjuvants would increase vaccine efficacy against fentanyl challenge, overdose, and self-administration in either rats or Hanford miniature pigs. Formulation of the vaccine with a nucleolipid TLR7/8 agonist enhanced its immunogenicity and efficacy in preventing fentanyl-induced respiratory depression, analgesia, bradycardia, and self-administration in either rats or mini-pigs. These studies support the use of TLR7/8 adjuvants in vaccine formulations to improve their clinical efficacy against OUD and potentially other substance use disorders (SUD).
© 2023. The Author(s).
Conflict of interest statement
MP is the co-inventor of patents disclosing fentanyl haptens reported in this manuscript (F1 or F, and F3), fentanyl hapten conjugates (F1-CRM, F-CRM), and methods for using them. JTE is a co-inventor of INI-4001 adjuvant, held the CEO position at Inimmune Corporation, and holds stock options in Inimmune Corporation. MP and JTE are co-inventors of patents disclosing formulations of fentanyl vaccines formulated with INI-4001. SMM is an employee of Inimmune Corporation and holds stock options in Inimmune Corporation. All other authors declare no competing interests.
Figures

References
-
- Centers for Disease Control and Prevention. N.C.f.I.P.a.C. Drug Overdose. (2021).
-
- Ahmad, F., Rossen, L. & Sutton, P. Provisional drug overdose death counts. National Center for Health Statistics. (2021).
-
- Control, C.F.D. Drug overdose deaths in the U.S. top 100,000 annually. Available from: https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2021/20211117.htm. (2021).
-
- Administration, S.A.a.M.H.S. MAT statutes, regulations, and guidelines. Available from: https://www.samhsa.gov/medication-assisted-treatment/statutes-regulation.... (2019)
Grants and funding
LinkOut - more resources
Full Text Sources
