

Myocardial strain-curve deformation patterns after Fontan operation
- PMID: 37488167
- PMCID: PMC10366156
- DOI: 10.1038/s41598-023-39226-y
Myocardial strain-curve deformation patterns after Fontan operation
Abstract
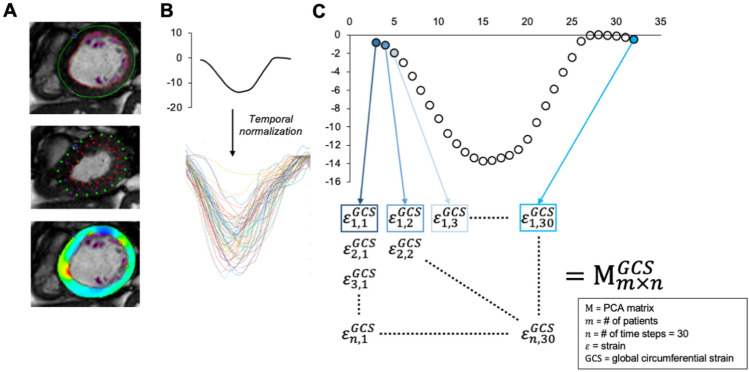
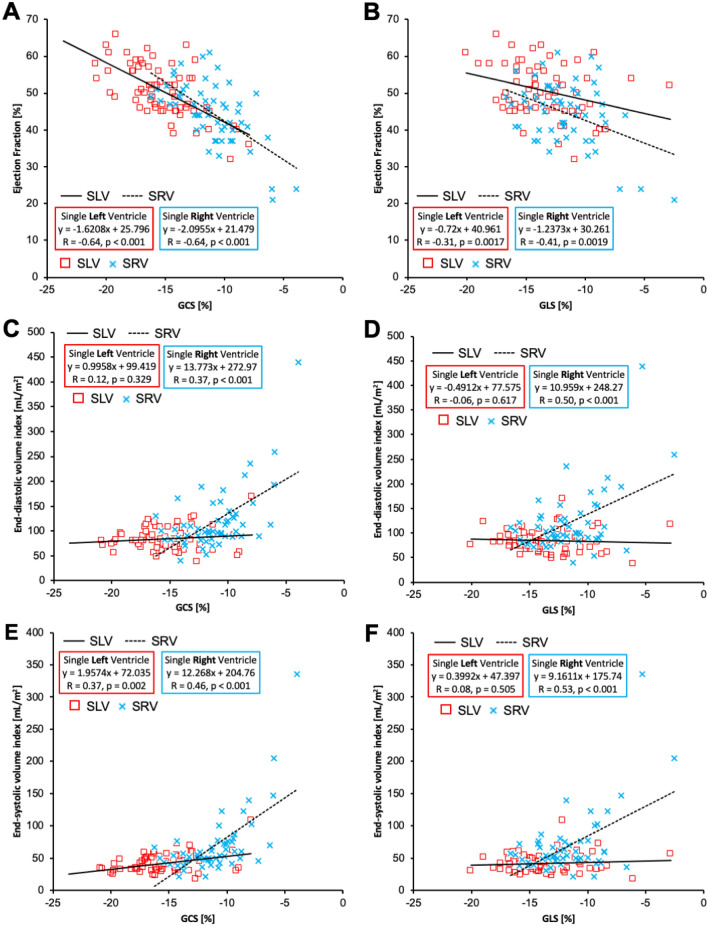
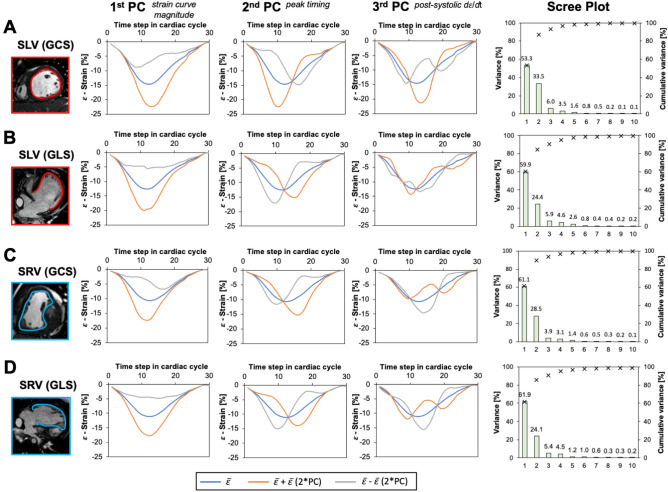
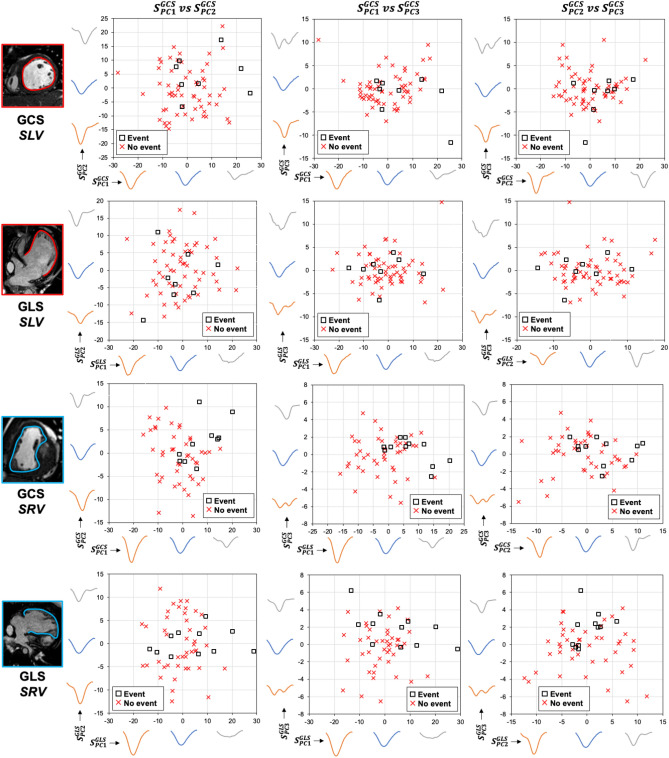
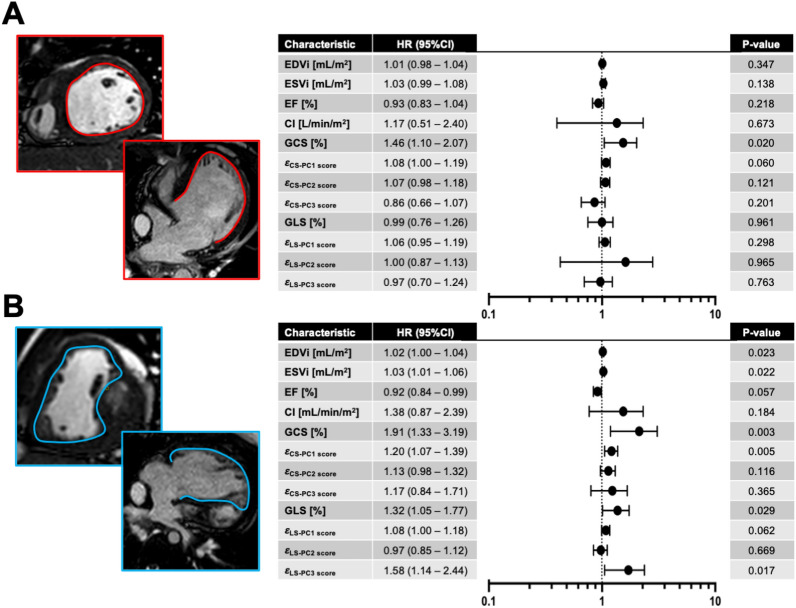
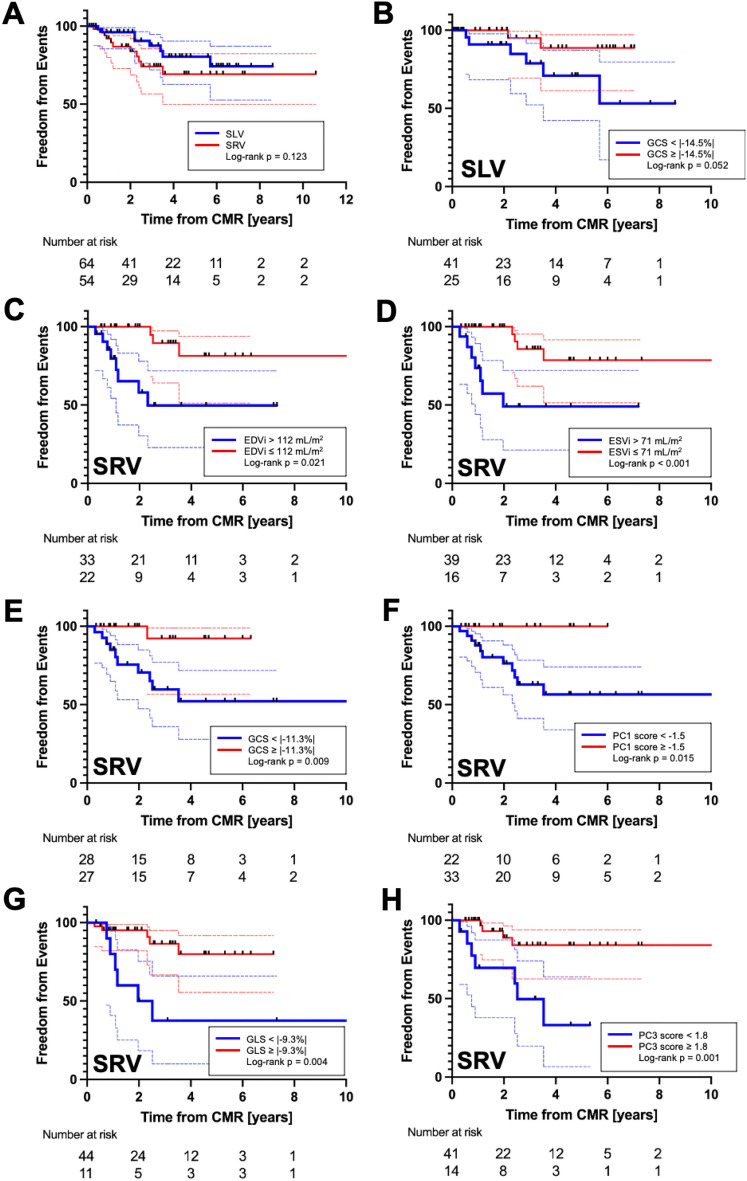
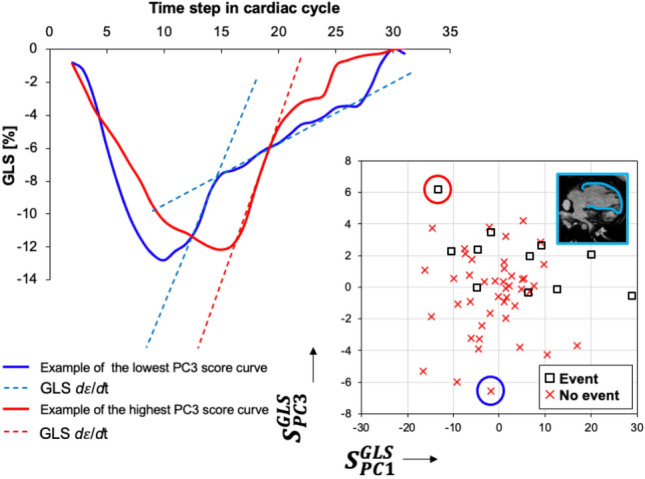
Myocardial deformation analysis by cardiac MRI (CMR) yielding global circumferential and longitudinal strain (GCS and GLS) is an increasingly utilized method to accurately quantify systolic function and predict clinical events in patients with Fontan circulation. The purpose of this study was to use principal component analysis (PCA) to investigate myocardial temporal deformation patterns derived from strain-time curves to learn about latent strain features beyond peak values. We conducted the study with specific attention to dominant single left or right ventricle (SLV and SRV) morphologies. Methods and Results: Patients remote from Fontan operation who underwent follow-up CMR were analyzed for standard volumetric and function hemodynamics including myocardial deformation parameters including GCS and GLS. We applied PCA to investigate in an unbiased fashion the strain-time curve morphology and to calculate patient specific shape scores. All variables were subjected to single variable Cox regression analysis to detect composite clinical outcome including death, heart transplant, protein losing enteropathy and plastic bronchitis. A total of 122 patients, (SLV = 67, SRV = 55) with a mean age of 12.7 years underwent comprehensive CMR analysis. The PCA revealed 3 primary modes of strain-curve variation regardless of single ventricle morphology and type of strain investigated. Principle components (PCs) described changes in (1) strain-time curve amplitude, (2) time-to-peak strain, and (3) post-systolic slope of the strain-time curve. Considering only SLV patients, GCS was only CMR variable predictive of clinical events (HR 1.46, p = 0.020). In the SRV group, significant CMR predictors of clinical events were derived indexed end-diastolic (HR 1.02, p = 0.023) and end-systolic (HR 1.03, p = 0.022) volumes, GCS (HR 1.91, p = 0.003) and its related first component score (HR 1.20, p = 0.005), GLS (HR 1.32, p = 0.029) and its third component score (HR 1.58, p = 0.017). CMR derived global strain measures are sensitive markers of clinical outcomes in patients with Fontan circulation, particularly in patients with the SRV morphology. Myocardial strain-time curve morphology specific to SLV and SRV patients inspired by unbiased PCA technique can further aid with predicting clinical outcomes.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Dardeer AM, Hudsmith L, Wesolowski R, Clift P, Steeds RP. The potential role of feature tracking in adult congenital heart disease: Advantages and disadvantages in measuring myocardial deformation by cardiovascular magnetic resonance. J. Congenit. Cardiol. 2018;21(2):1–11.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
