

Dose escalation and expansion cohorts in patients with advanced breast cancer in a Phase I study of the CDK7-inhibitor samuraciclib
- PMID: 37488191
- PMCID: PMC10366102
- DOI: 10.1038/s41467-023-40061-y
Dose escalation and expansion cohorts in patients with advanced breast cancer in a Phase I study of the CDK7-inhibitor samuraciclib
Erratum in
-
Author Correction: Dose escalation and expansion cohorts in patients with advanced breast cancer in a Phase I study of the CDK7-inhibitor samuraciclib.Nat Commun. 2023 Aug 7;14(1):4741. doi: 10.1038/s41467-023-40561-x. Nat Commun. 2023. PMID: 37550302 Free PMC article. No abstract available.
-
Author Correction: Dose escalation and expansion cohorts in patients with advanced breast cancer in a Phase I study of the CDK7-inhibitor samuraciclib.Nat Commun. 2025 Mar 6;16(1):2242. doi: 10.1038/s41467-025-57535-w. Nat Commun. 2025. PMID: 40050276 Free PMC article. No abstract available.
Abstract
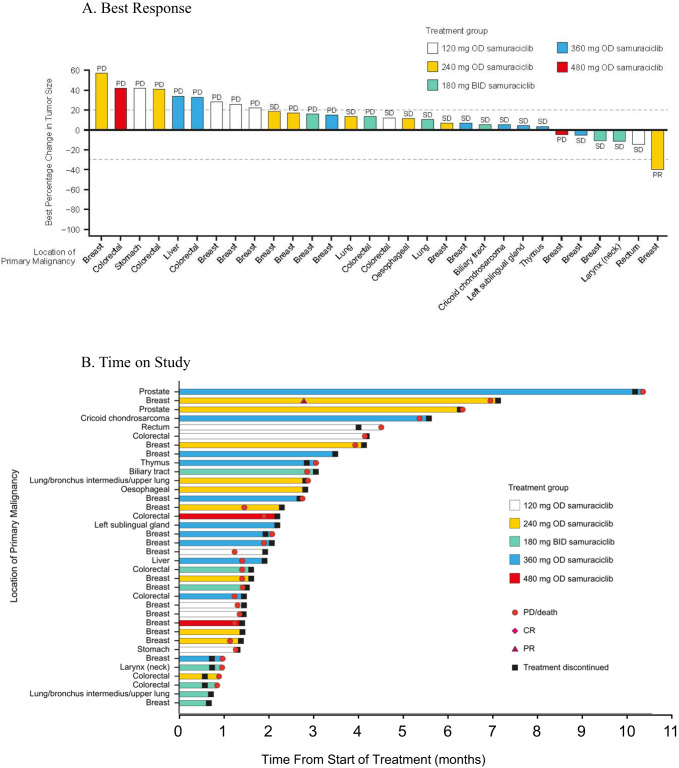
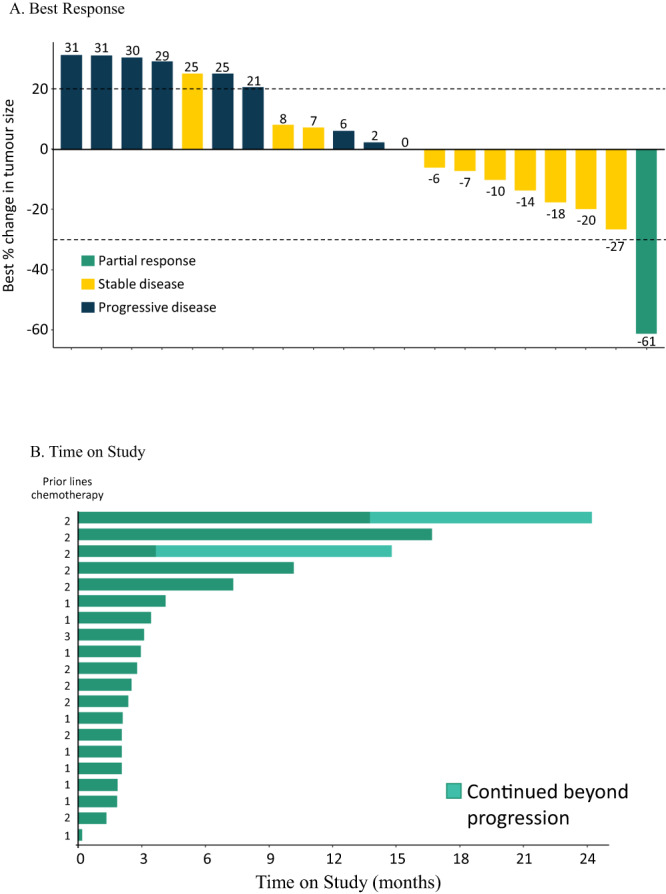
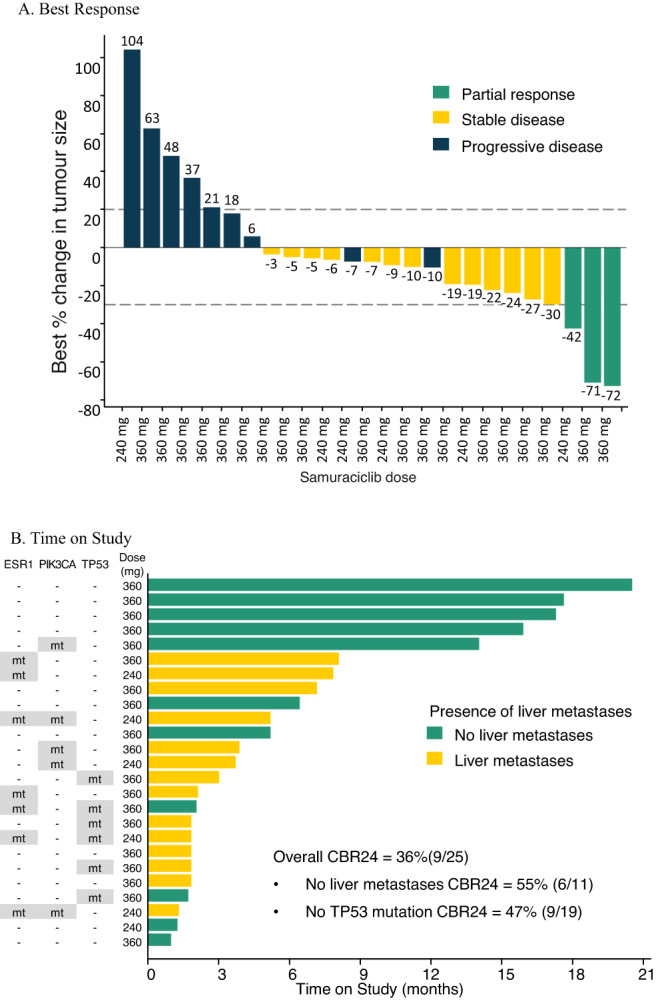
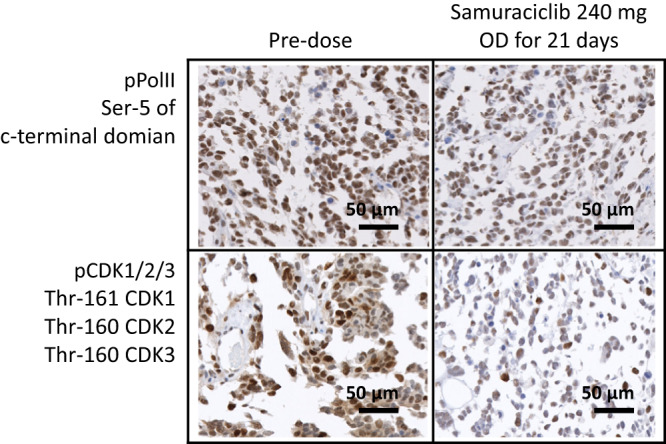
Samuraciclib is a selective oral CDK7-inhibitor. A multi-modular, open-label Phase I study to evaluate safety and tolerability of samuraciclib in patients with advanced malignancies was designed (ClinicalTrials.gov: NCT03363893). Here we report results from dose escalation and 2 expansion cohorts: Module 1A dose escalation with paired biopsy cohort in advanced solid tumor patients, Module 1B-1 triple negative breast cancer (TNBC) monotherapy expansion, and Module 2A fulvestrant combination in HR+/HER2- breast cancer patients post-CDK4/6-inhibitor. Core study primary endpoints are safety and tolerability, and secondary endpoints are pharmacokinetics (PK), pharmacodynamic (PD) activity, and anti-tumor activity. Common adverse events are low grade nausea, vomiting, and diarrhea. Maximum tolerated dose is 360 mg once daily. PK demonstrates dose proportionality (120 mg-480 mg), a half-life of approximately 75 hours, and no fulvestrant interaction. In dose escalation, one partial response (PR) is identified with disease control rate of 53% (19/36) and reduction of phosphorylated RNA polymerase II, a substrate of CDK7, in circulating lymphocytes and tumor tissue. In TNBC expansion, one PR (duration 337 days) and clinical benefit rate at 24 weeks (CBR) of 20.0% (4/20) is achieved. In combination with fulvestrant, 3 patients achieve PR with CBR 36.0% (9/25); in patients without detectable TP53-mutation CBR is 47.4% (9/19). In this study, samuraciclib exhibits tolerable safety and PK is supportive of once-daily oral administration. Clinical activity in TNBC and HR+/HER2-breast cancer post-CDK4/6-inhibitor settings warrants further evaluation.
© 2023. The Author(s).
Conflict of interest statement
R.C.C. has had a travel grant from Carrick Therapeutics and owns a patent on samuraciclib (patent number WO/2015/124941); he also has a grant from AstraZeneca. S.H. has received speaker fees Pfizer and advisory board and grant funding from Lilly. S.R.L. has received consulting fees from Sanofi, GLG consulting, Atheneum and Rejuversen. He has also received payment or honoraria for lectures, presentations, or educational events from Eisai, Prosigna, Roche, Pfizer, Novartis, Shionogi and Sanofi, and was previously employed by Pfizer. He has received travel, accommodation or expenses from Pfizer, Roche, Synthon and Piqur Therapeutics, and research funding from CRUK, Against Breast Cancer, Pathios Therapeutics and is cofounder of Mitox Therapeutics. His institution has received funding for clinical trials for which he was chief/principal investigator from CRUK, Boehringer Ingelheim, Piqur Therapeutics, Astra Zeneca, Carrick Therapeutics, Sanofi, Merck KGaA, Synthon, Roche and Prostate Cancer UK. J.O. has received honoraria for consulting and/or advisory boards from the following: AbbVie Inc., Agendia, Amgen Biotechnology, Aptitude Health, AstraZeneca, Bayer, Bristol-Myers Squibb, Carrick Therapeutics, Celgene Corporation, Clovis Oncology, Daiichi Sankyo, Eisai, G1 Therapeutics, Genentech, Gilead Sciences, GRAIL, Halozyme Therapeutics, Heron Therapeutics, Immunomedics, Ipsen Biopharmaceuticals, Lilly, Merck, Myriad, Nektar Therapeutics, Novartis, Ontada, Pfizer, Pharmacyclics, Pierre Fabre Pharmaceuticals, Puma Biotechnology, Prime Oncology, Roche, Samsung Bioepis, Sanofi, Seagen, Syndax Pharmaceuticals, Taiho Oncology, Takeda, and Synthon. ZM has a consulting/advisory role with AstraZeneca, Gilead Sciences and Daiichi Sankyo. He has also received research funding for his institution from Seattle Genetics, Novartis, AstraZeneca, Radius Health, Daiichi Sankyo, Lilly, GlaxoSmithKline, and Olema Oncology. CP acknowledges support from The Liverpool Experimental Cancer Medicine Centre [Grant Reference:C18616/A25153], The Clatterbridge Cancer Charity, North West Cancer and Make 2nds Count. CP reports grant funding support from Pfizer, Daiichi Sankyo, Exact Sciences, Gilead and Seagen. Honoraria for advisory boards have been received from Pfizer, Roche, Daiichi Sankyo, Novartis, Exact sciences, Gilead, SeaGen and Eli Lilly and support for travel and conferences from Roche, Novartis and Gilead. T.A. is employed by Sarah Cannon/HCA Healthcare UK and Ellipses Pharma and receives funding in an advisory capacity from iOnctura, Labgenius, and Servier. R.D.B. has a consulting/advisory role with Shionogi, Daiichi Sankyo, Molecular Partners, Roche/Genentech, Novartis, and AstraZeneca. He has also received research funding for his institution from AstraZeneca, Genentech, Shionogi, Molecular Partners, Sanofi, Boehringer Ingelheim, Roche, Biomarin, GI Therapeutics, and Carrick Therapeutics, and travel/accommodation/expenses from Shionogi, AstraZeneca, Molecular Partners, and Daiichi Sankyo. R.J. has received research funding from Pfizer and Lilly, and she serves on an advisory board for Carrick Therapeutics and Luminex. S.A. is a named inventor on patents describing CDK inhibitors, including samuraciclib, owns shares in Carrick Therapeutics and has been funded by Carrick Therapeutics; he also has grants from AstraZeneca. G.C., A.B., and S.M. are Carrick employees and shareholders. M.K. has received honoraria from Janssen, Roche; consulting/advisory fees from Achilles Therapeutics, Bayer, Guardant Health, Janssen, OM Pharma, Roche, Seattle Genetics; speakers fees from AstraZeneca, Janssen, Roche and research funding from Roche and Novartis for his institution. He has received travel, accommodation or expenses from AstraZeneca, BerGenBio, Immutep, Janssen and Roche. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
