

Acoustic and optoacoustic stimulations in auditory brainstem response test in salicylate induced tinnitus
- PMID: 37488197
- PMCID: PMC10366222
- DOI: 10.1038/s41598-023-39033-5
Acoustic and optoacoustic stimulations in auditory brainstem response test in salicylate induced tinnitus
Abstract
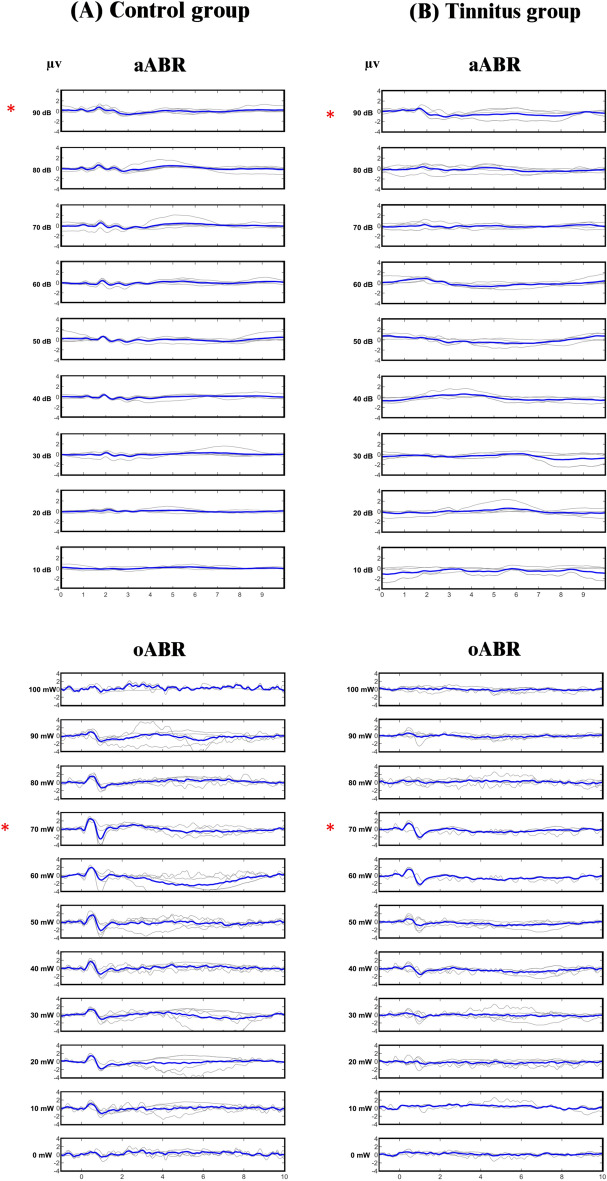
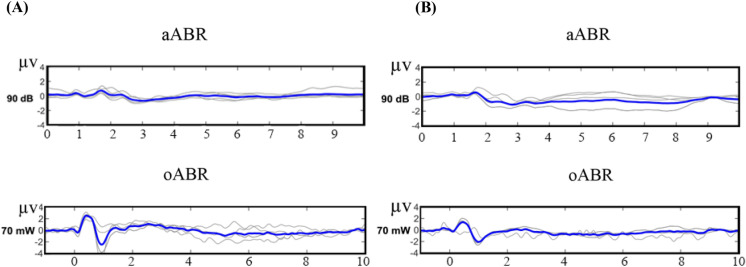
As a common debilitating disorder worldwide, tinnitus requires objective assessment. In the auditory brainstem response (ABR) test, auditory potentials can be evoked by acoustic or optoacoustic (induced by laser light) stimulations. In order to use the ABR test in the objective assessment of tinnitus, in this study, acoustic ABR (aABR) and optoacoustic ABR (oABR) were compared in the control and tinnitus groups to determine the changes caused by sodium salicylate (SS)-induced tinnitus in rat. In both aABR and oABR, wave II was the most prominent waveform, and the amplitude of wave II evoked by oABR was significantly higher than that of aABR. Brainstem transmission time (BTT), which represents the time required for a neural stimulation to progress from the auditory nerve ending to the inferior colliculus, was significantly shorter in oABR. In the tinnitus group, there was a significant increase in the threshold of both ABRs and a significant decrease in the amplitude of wave II only in the oABR. Based on our findings, the ABR test has the potential to be used in the assessment of SS-induced tinnitus, but oABR has the advantages of producing more prominent waveforms and significantly reducing the amplitude of wave II in tinnitus.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
