

Comparison of Four-Dimensional Flow MRI, Two-Dimensional Phase-Contrast MRI and Echocardiography in Transposition of the Great Arteries
- PMID: 37488239
- PMCID: PMC11442473
- DOI: 10.1007/s00246-023-03238-2
Comparison of Four-Dimensional Flow MRI, Two-Dimensional Phase-Contrast MRI and Echocardiography in Transposition of the Great Arteries
Abstract
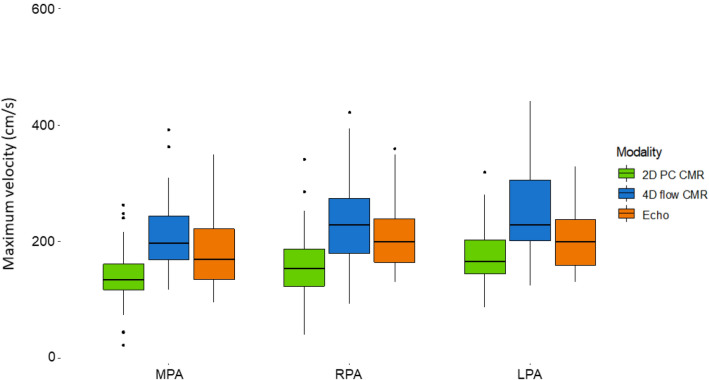
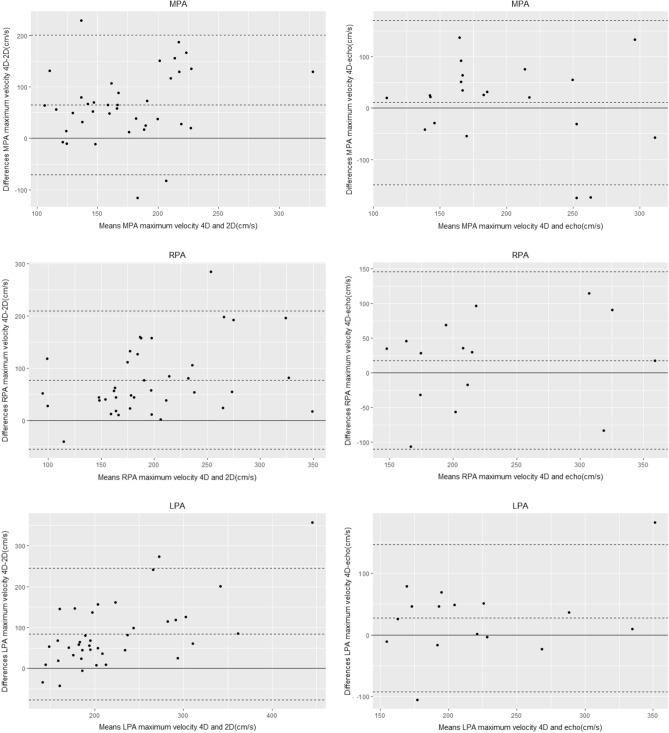
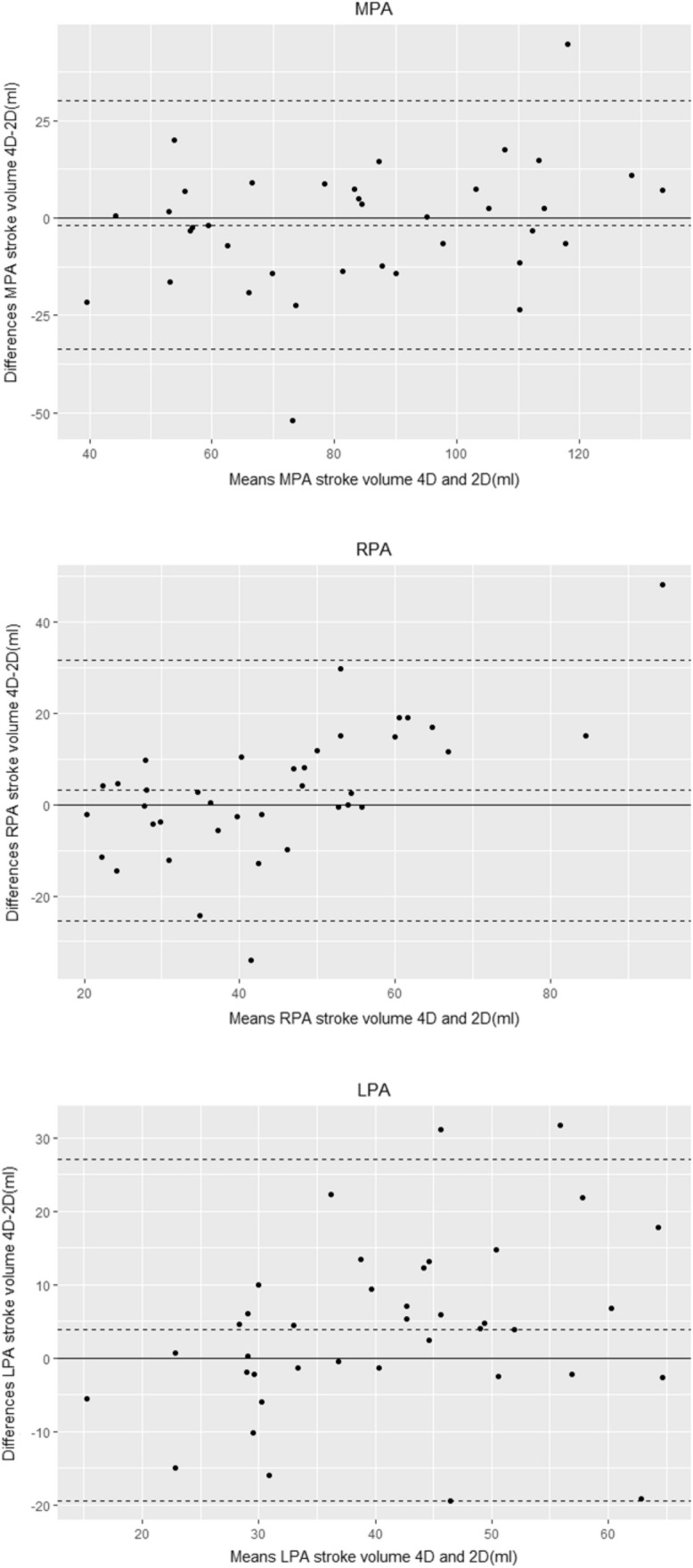
Pulmonary artery (PA) stenosis is a common complication after the arterial switch operation (ASO) for transposition of the great arteries (TGA). Four-dimensional flow (4D flow) CMR provides the ability to quantify flow within an entire volume instead of a single plane. The aim of this study was to compare PA maximum velocities and stroke volumes between 4D flow CMR, two-dimensional phase-contrast (2D PCMR) and echocardiography. A prospective study including TGA patients after ASO was performed between December 2018 and October 2020. All patients underwent echocardiography and CMR, including 2D PCMR and 4D flow CMR. Maximum velocities and stroke volumes were measured in the main, right, and left PA (MPA, LPA, and RPA, respectively). A total of 39 patients aged 20 ± 8 years were included. Maximum velocities in the MPA, LPA, and RPA measured by 4D flow CMR were significantly higher compared to 2D PCMR (p < 0.001 for all). PA assessment by echocardiography was not possible in the majority of patients. 4D flow CMR maximum velocity measurements were consistently higher than those by 2D PCMR with a mean difference of 65 cm/s for the MPA, and 77 cm/s for both the RPA and LPA. Stroke volumes showed good agreement between 4D flow CMR and 2D PCMR. Maximum velocities in the PAs after ASO for TGA are consistently lower by 2D PCMR, while echocardiography only allows for PA assessment in a minority of cases. Stroke volumes showed good agreement between 4D flow CMR and 2D PCMR.
Keywords: Advanced cardiac imaging; Congenital heart disease; Magnetic resonance imaging; Transposition of the great arteries.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Morgan CT, Mertens L, Grotenhuis HB, Yoo SJ, Seed M, Grosse-Wortmann L (2017) Understanding the mechanism for branch pulmonary artery stenosis after the arterial switch operation for transposition of the great arteries. Eur Heart J Cardiovasc Imaging 18(2):180–185. 10.1093/ehjci/jew046 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
