

Neoadjuvant adebrelimab in locally advanced resectable esophageal squamous cell carcinoma: a phase 1b trial
- PMID: 37488287
- PMCID: PMC10427424
- DOI: 10.1038/s41591-023-02469-3
Neoadjuvant adebrelimab in locally advanced resectable esophageal squamous cell carcinoma: a phase 1b trial
Erratum in
-
Publisher Correction: Neoadjuvant adebrelimab in locally advanced resectable esophageal squamous cell carcinoma: a phase 1b trial.Nat Med. 2023 Sep;29(9):2376. doi: 10.1038/s41591-023-02511-4. Nat Med. 2023. PMID: 37507607 Free PMC article. No abstract available.
Abstract
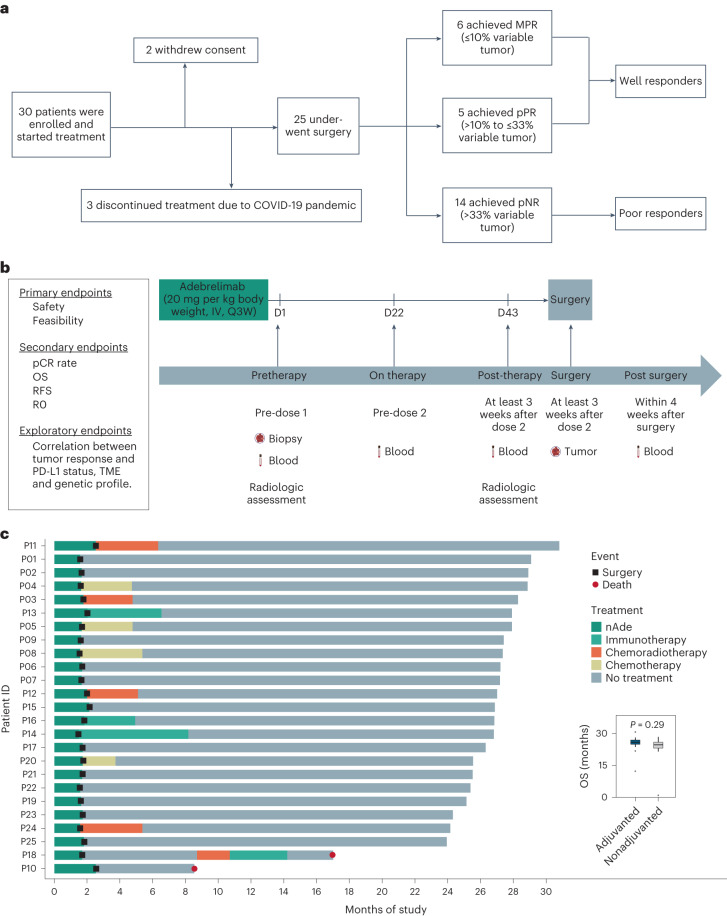
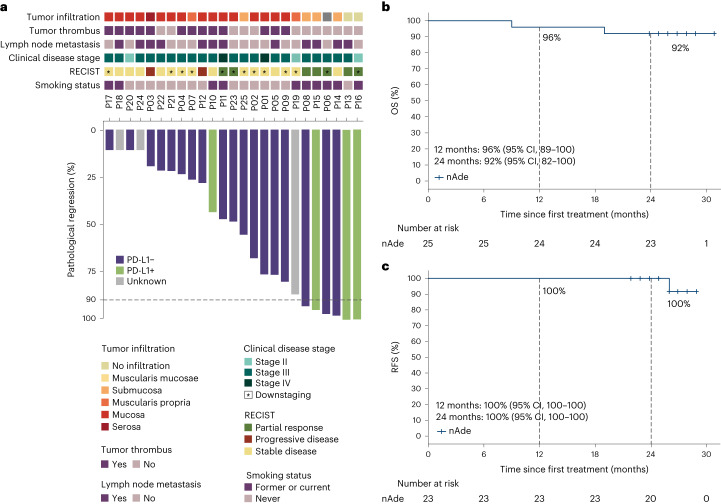
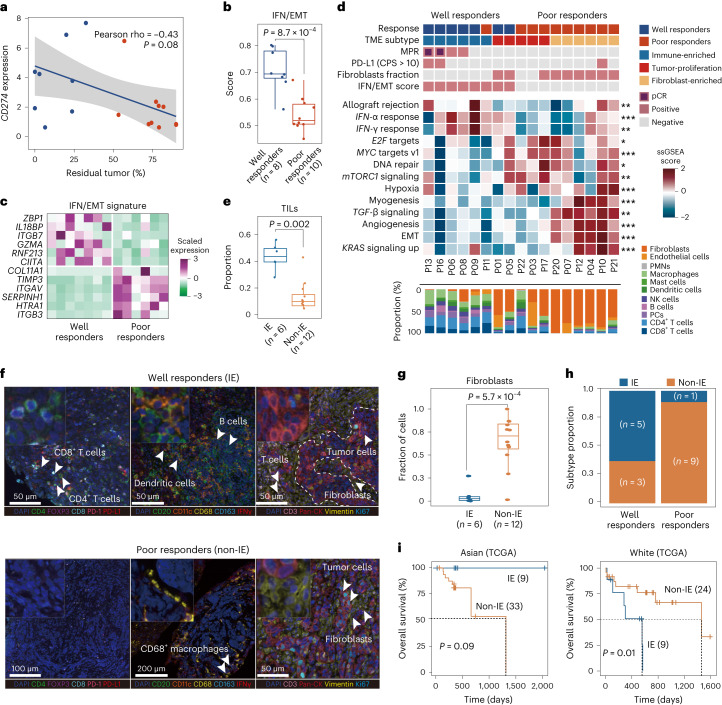
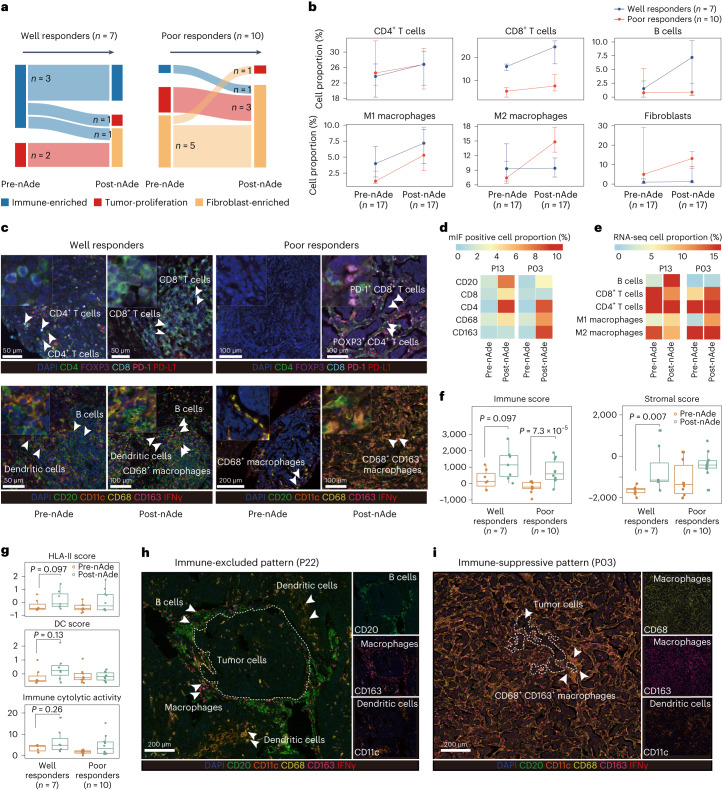
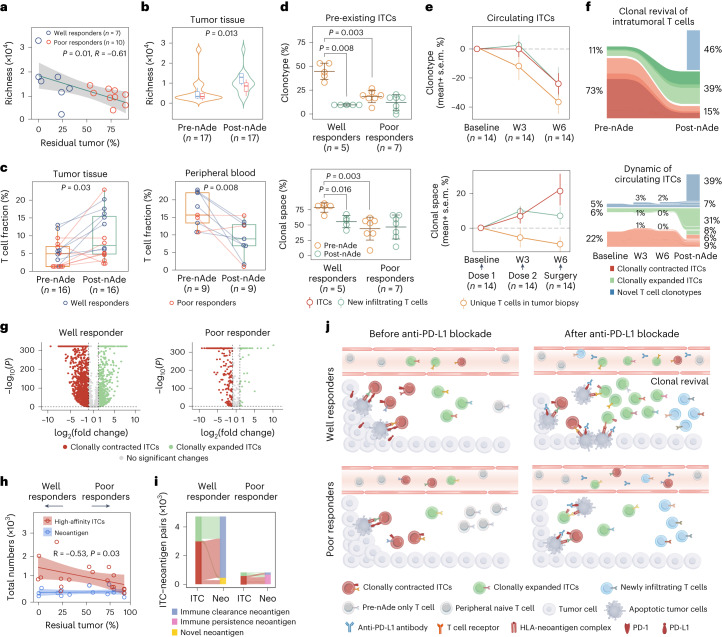
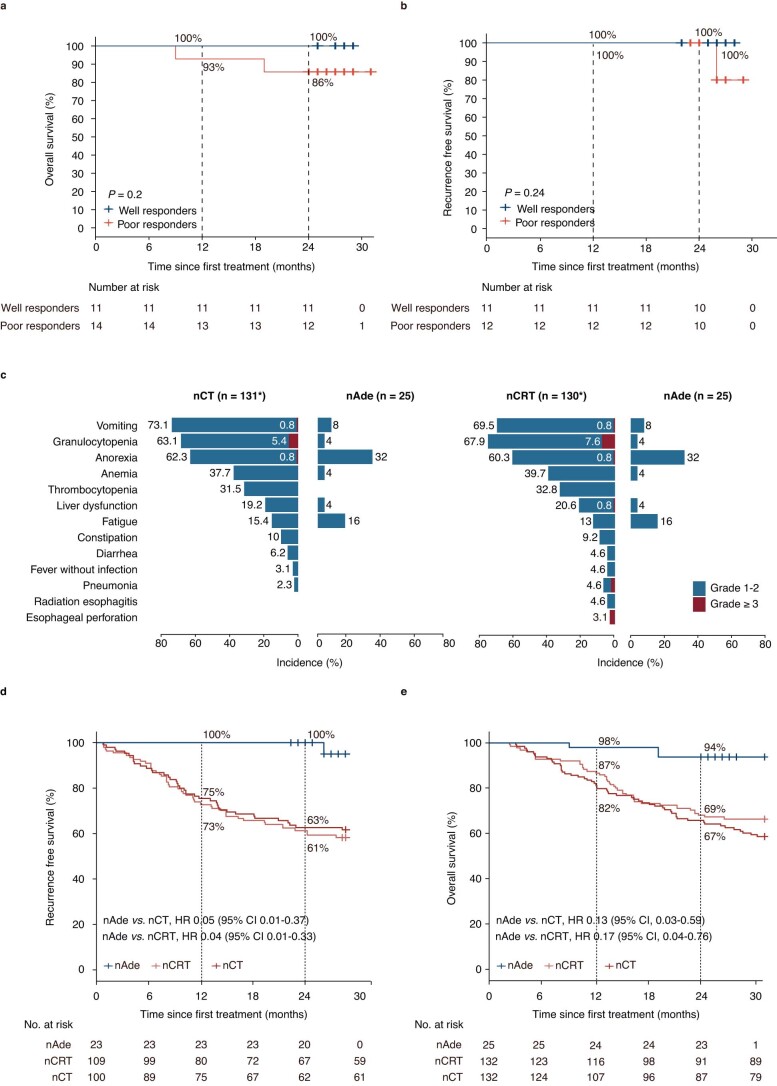
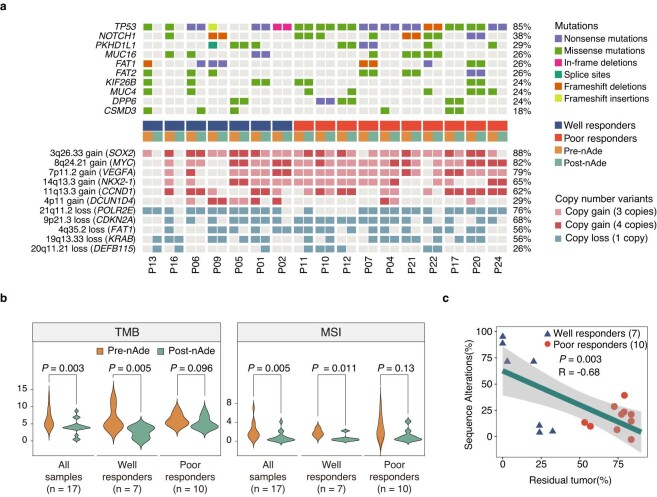
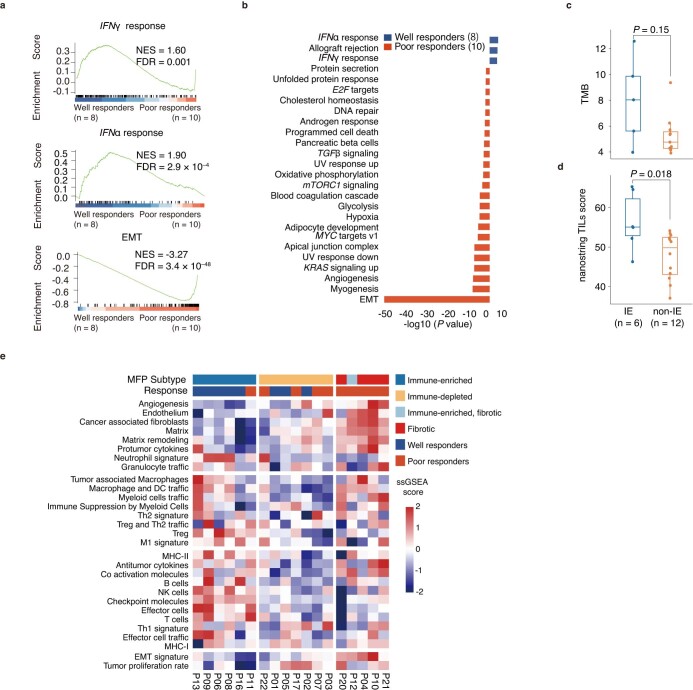
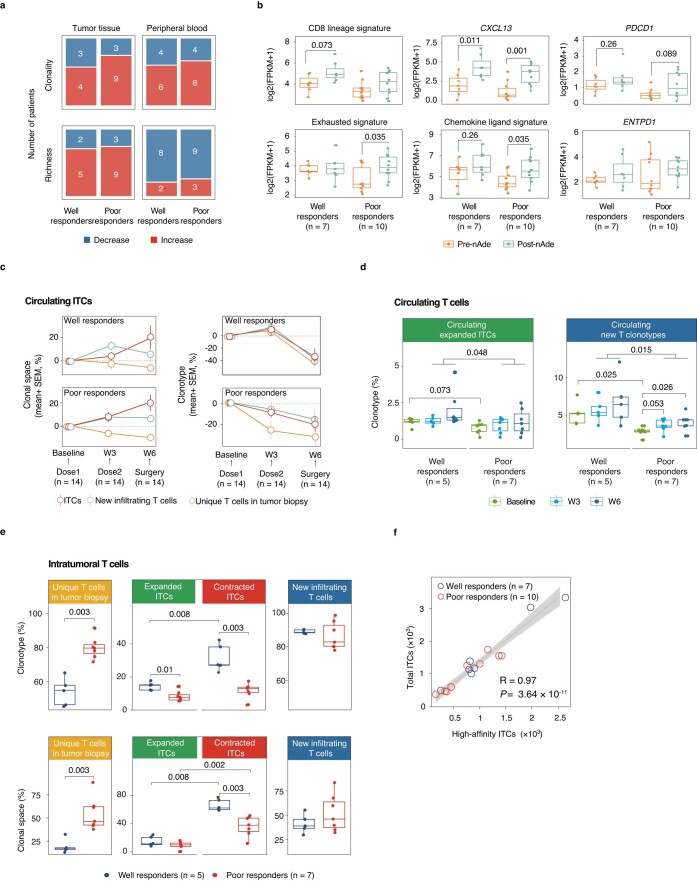
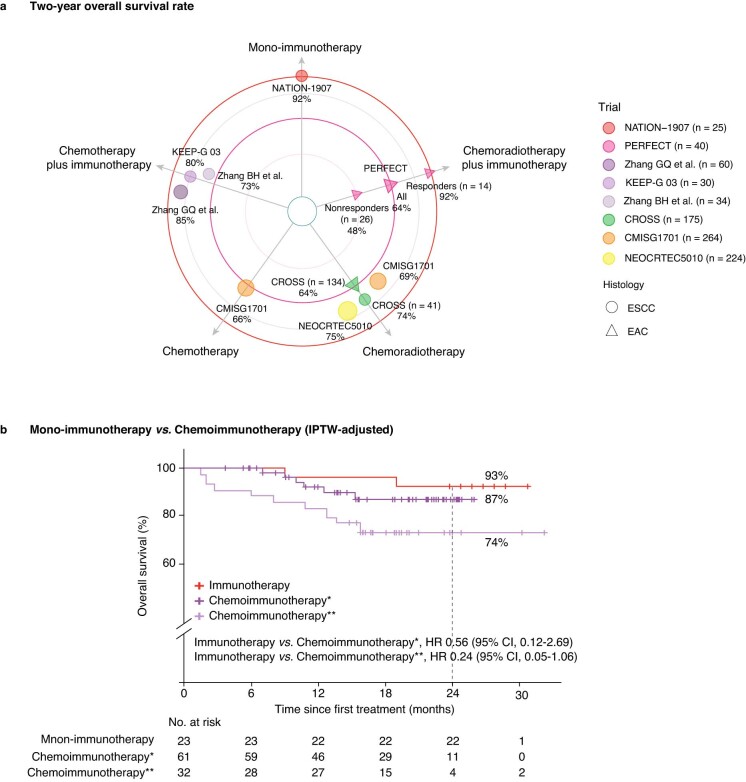
Overall survival (OS) benefits of neoadjuvant immunotherapy remain elusive in locally advanced esophageal squamous cell carcinomas (ESCC). Here, we reported the results of a phase 1b trial of neoadjuvant PD-L1 blockade with adebrelimab in resectable ESCC. Patients received two neoadjuvant doses of adebrelimab followed by surgery. The primary endpoints were safety and feasibility; secondary endpoints included pathologic complete response (pCR) and OS. Our data showed the primary endpoints of safety and feasibility had been met. Common treatment-related adverse events were anorexia (32%) and fatigue (16%), without grade 3 or more adverse events. Of the 30 patients enrolled in the trial, 25 underwent successful resection without surgery delay and 24% had major pathologic responses including a pCR rate of 8%. The 2-year OS was 92%. Responsive patients had an immune-enriched tumor microenvironment phenotype, whereas nonresponsive patients had greater infiltration of cancer-associated fibroblasts at baseline. Clonotypic dynamics of pre-existing intratumoral T cells was a hallmark of responsive patients. These findings provide a rational for neoadjuvant anti-PD-L1 monotherapy as a therapeutic strategy for patients with resectable ESCC. ClinicalTrials.gov identifier: NCT04215471 .
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Tang H, et al. Neoadjuvant chemoradiotherapy versus neoadjuvant chemotherapy followed by minimally invasive esophagectomy for locally advanced esophageal squamous cell carcinoma: a prospective multicenter randomized clinical trial. Ann. Oncol. 2023;34:163–172. doi: 10.1016/j.annonc.2022.10.508. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
