

Pathogenesis of spinal intramedullary lipomas: two case reports
- PMID: 37488574
- PMCID: PMC10367250
- DOI: 10.1186/s13256-023-04048-z
Pathogenesis of spinal intramedullary lipomas: two case reports
Abstract
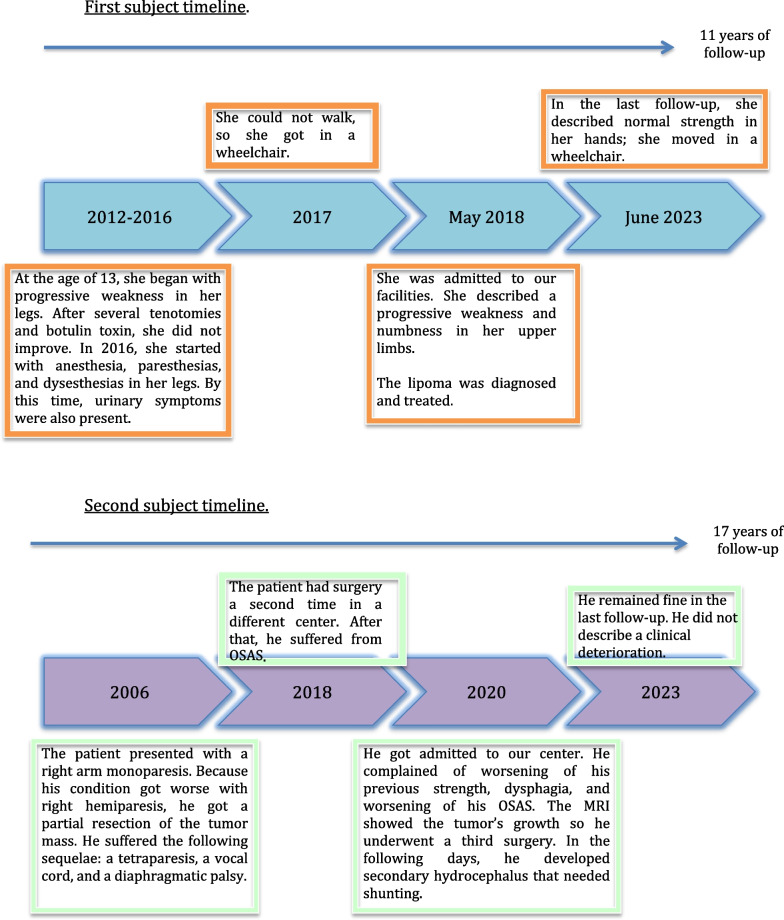
Background: Spinal lipomas not associated with dysraphism are rare and have an unknown natural history. In this report, we describe two cases; they showed recurrence during long-term follow-up, which makes us doubt a benign malformative etiology.
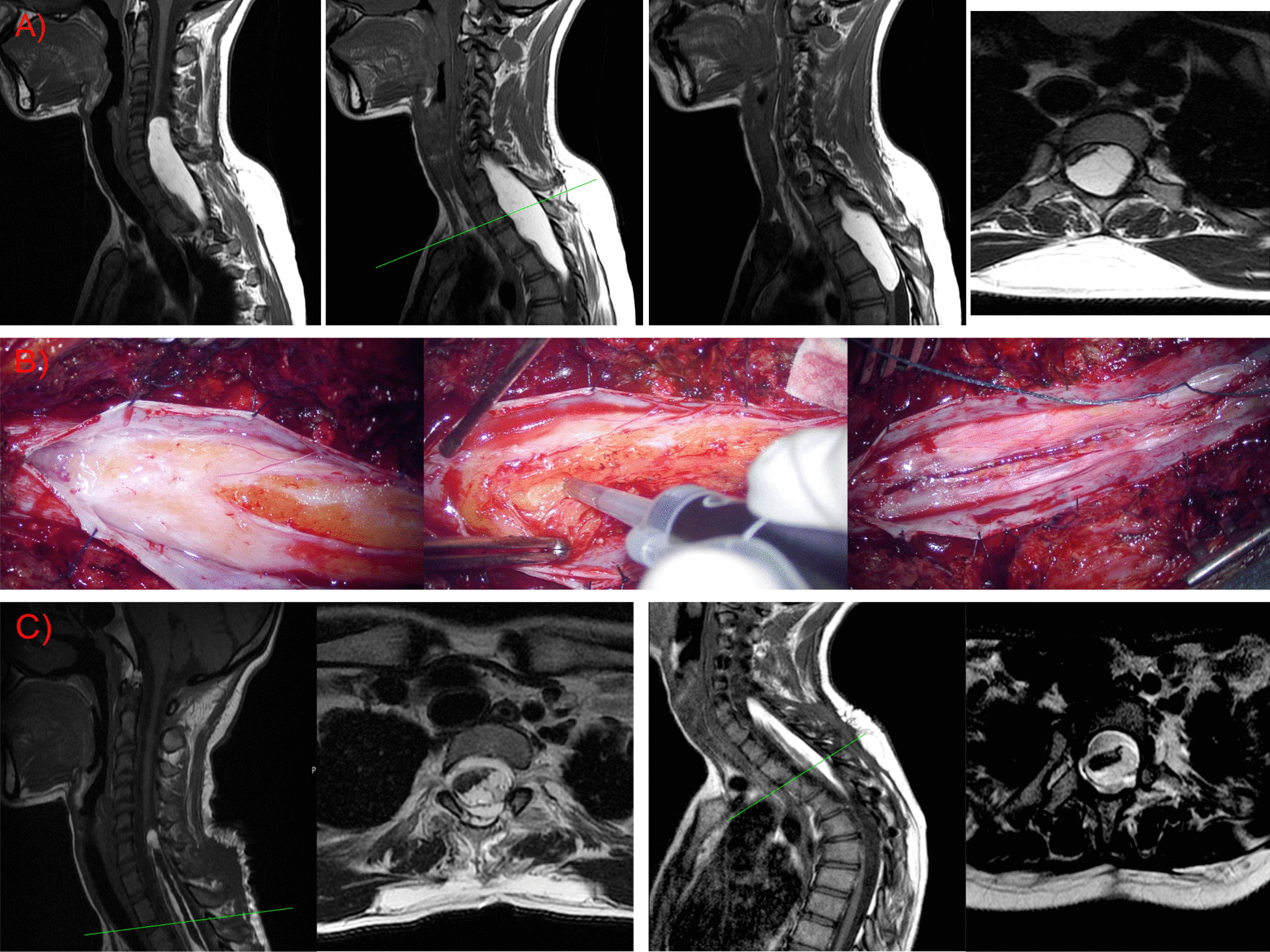
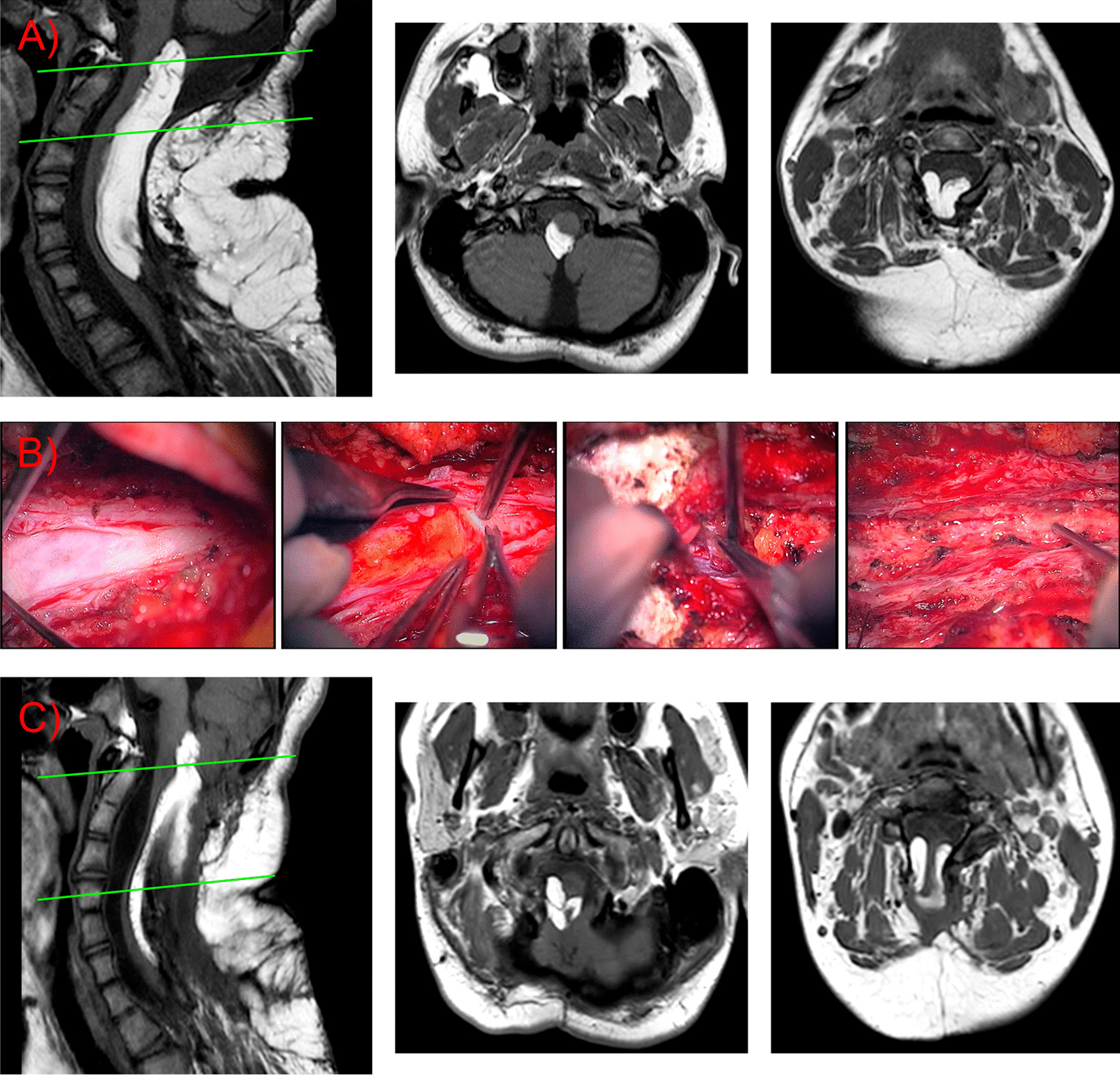
Case reports: Two patients, a 19-year-old South American woman and a 14-year-old boy with spinal lipomas, underwent surgical resection. The lipomas were not associated with dysraphism and were located in the cervicothoracic and craniocervical junctions. In both cases, we decided to operate due to clinical progression; the former had a progressive natural course, and the latter experienced clinical worsening after recurrence from previous surgeries. The surgery took place with the assistance of neurophysiological monitoring and intraoperative ultrasound; a partial resection and medullary decompression were done, following the more recent recommendations.
Discussion: The natural history of these lesions is currently unknown due to their rarity and the heterogeneity in the long-term follow-up of previously reported cases. Although previous reports describe good outcomes after surgical resection, long follow-ups, especially in young subjects, may show differences in these outcomes with progression and recurrence. We contribute to this last piece of evidence by describing two more cases of progression and recurrence.
Lessons: Long-term close follow-up should be done in young subjects with spinal lipomas, as they are more prone to an aggressive course. Metabolism and hormonal changes may be behind this progression. Reoperation must be considered if neurological decline is detected.
Keywords: Dysraphism; Lipomas; Malformation; Metabolism; Recurrence; Spine.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
