

Worldwide trends in esophageal cancer survival, by sub-site, morphology, and sex: an analysis of 696,974 adults diagnosed in 60 countries during 2000-2014 (CONCORD-3)
- PMID: 37488785
- PMCID: PMC10508138
- DOI: 10.1002/cac2.12457
Worldwide trends in esophageal cancer survival, by sub-site, morphology, and sex: an analysis of 696,974 adults diagnosed in 60 countries during 2000-2014 (CONCORD-3)
Abstract
Background: Esophageal cancer survival is poor worldwide, though there is some variation. Differences in the distribution of anatomical sub-site and morphological sub-type may help explain international differences in survival for all esophageal cancers combined. We estimated survival by anatomic sub-site and morphological sub-type to understand further the impact of topography and morphology on international comparisons of esophageal cancer survival.
Methods: We estimated age-standardized one-year and five-year net survival among adults (15-99 years) diagnosed with esophageal cancer in each of 60 participating countries to monitor survival trends by calendar period of diagnosis (2000-2004, 2005-2009, 2010-2014), sub-site, morphology, and sex.
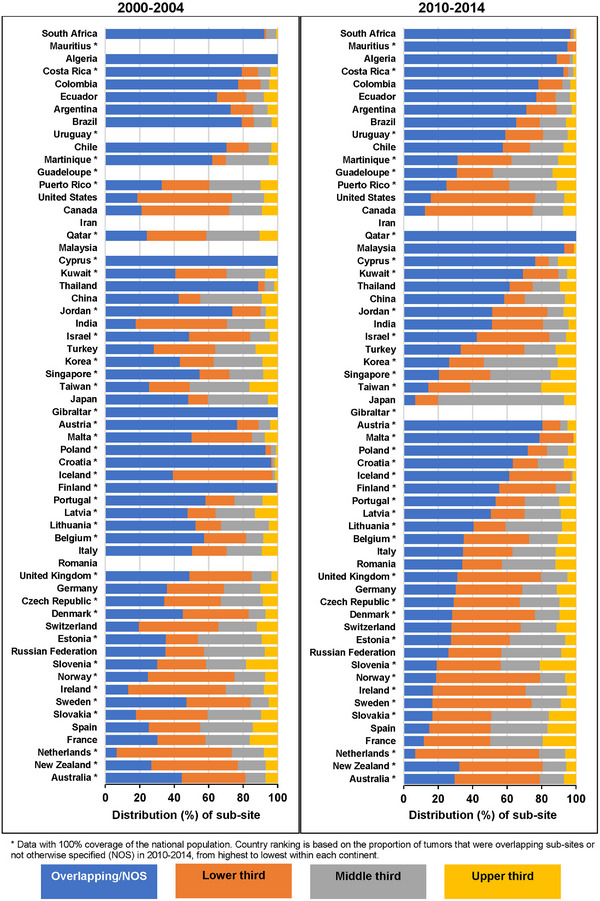
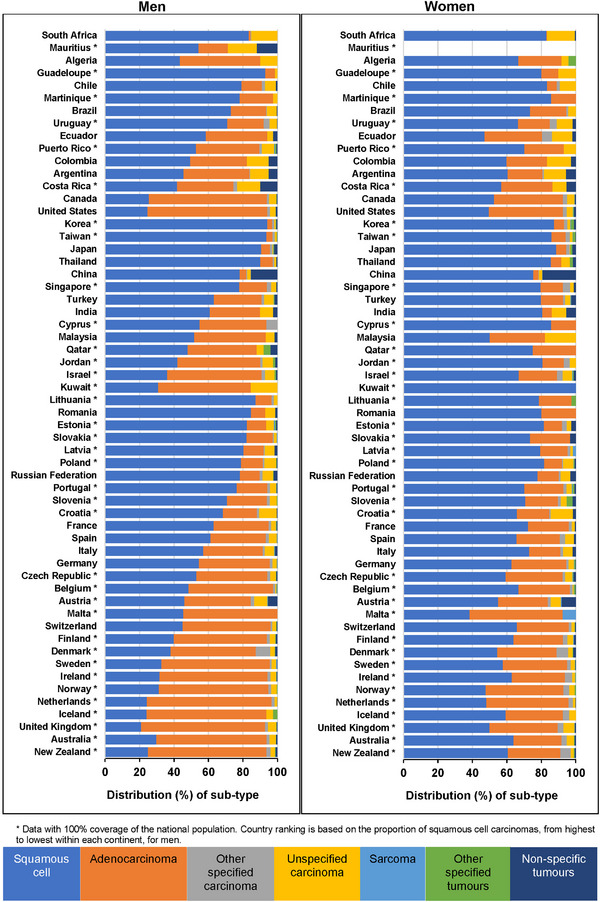
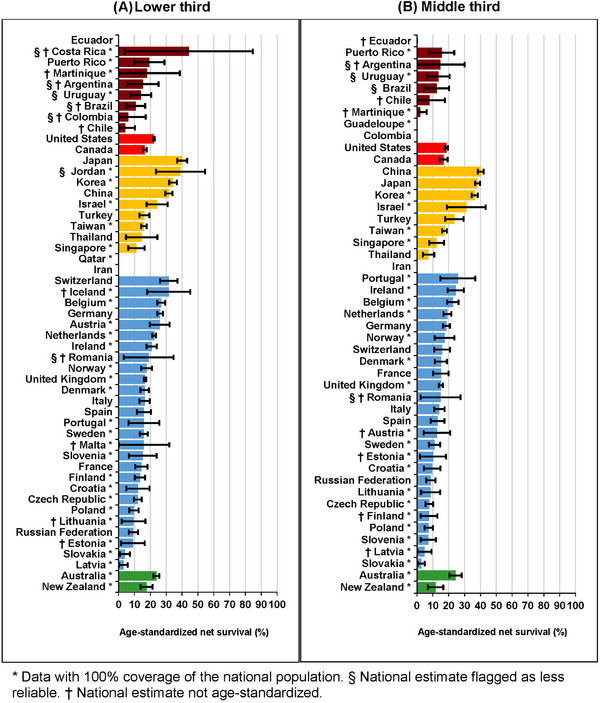
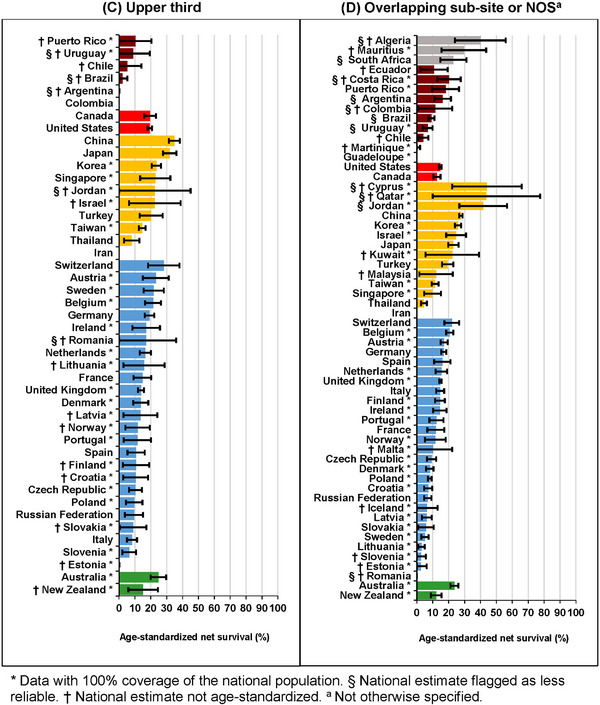
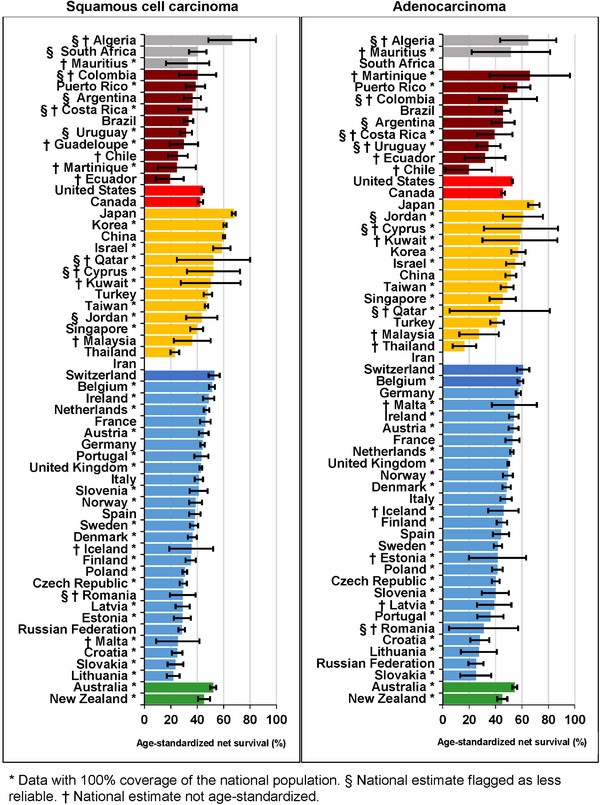
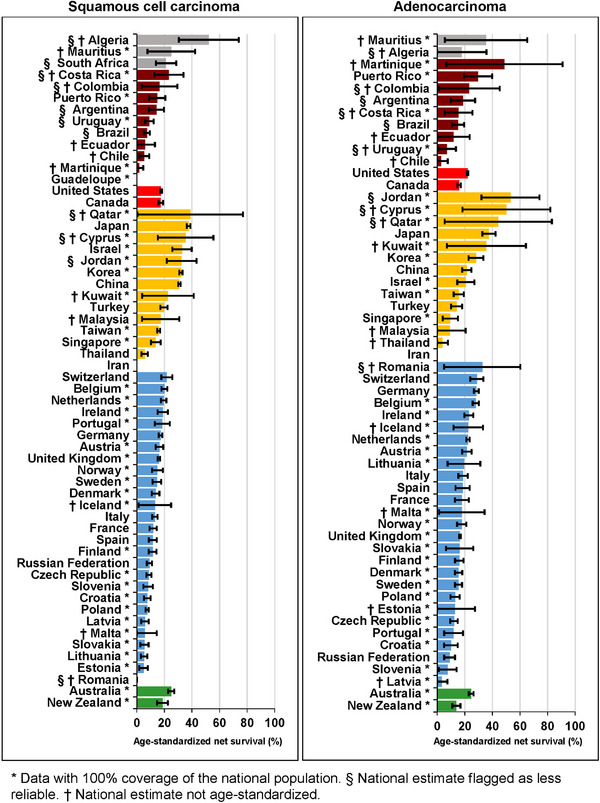
Results: For adults diagnosed during 2010-2014, tumors in the lower third of the esophagus were the most common, followed by tumors of overlapping sub-site and sub-site not otherwise specified. The proportion of squamous cell carcinomas diagnosed during 2010-2014 was generally higher in Asian countries (50%-90%), while adenocarcinomas were more common in Europe, North America and Oceania (50%-60%). From 2000-2004 to 2010-2014, the proportion of squamous cell carcinoma generally decreased, and the proportion of adenocarcinoma increased. Over time, there were few improvements in age-standardized five-year survival for each sub-site. Age-standardized one-year survival was highest in Japan for both squamous cell carcinoma (67.7%) and adenocarcinoma (69.0%), ranging between 20%-60% in most other countries. Age-standardized five-year survival from squamous cell carcinoma and adenocarcinoma was similar for most countries included, around 15%-20% for adults diagnosed during 2010-2014, though international variation was wider for squamous cell carcinoma. In most countries, survival for both squamous cell carcinoma and adenocarcinoma increased by less than 5% between 2000-2004 and 2010-2014.
Conclusions: Esophageal cancer survival remains poor in many countries. The distributions of sub-site and morphological sub-type vary between countries, but these differences do not fully explain international variation in esophageal cancer survival.
Keywords: Cancer; esophagus; morphology; survival; topography; trends.
© 2023 The Authors. Cancer Communications published by John Wiley & Sons Australia, Ltd. on behalf of Sun Yat-sen University Cancer Center.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000‐14 (CONCORD‐3): analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population‐based registries in 71 countries. The Lancet. 2018;391(10125):1023–75. - PMC - PubMed
-
- Lagergren J, Smyth E, Cunningham D, Lagergren P. Oesophageal cancer. The Lancet. 2017;390(10110):2383–96. - PubMed
-
- Schottenfeld D, Fraumeni JF. Cancer epidemiology and prevention. 3rd ed. Oxford; New York: Oxford University Press; 2006. xviii, 1392 p. p.
-
- Crane LM, Schaapveld M, Visser O, Louwman MW, Plukker JT, van Dam GM. Oesophageal cancer in The Netherlands: increasing incidence and mortality but improving survival. European Journal of Cancer. 2007;43(9):1445–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
