

The thicker the endometrium, the better the neonatal outcomes?
- PMID: 37489142
- PMCID: PMC10363027
- DOI: 10.1093/hropen/hoad028
The thicker the endometrium, the better the neonatal outcomes?
Abstract
Study question: Is endometrial thickness (EMT) on the hCG trigger day related to the neonatal outcome of a single birth after fresh embryo transfer (ET)?
Summary answer: An EMT ≤7.8 mm was an independent predictor for greater odds of preterm delivery (PTD) of singletons born after fresh ET.
What is known already: There may be a positive association between live birth rates and EMT after fresh ET. It is still unknown whether a similar association is seen for the neonatal outcomes of singletons in fresh cycles.
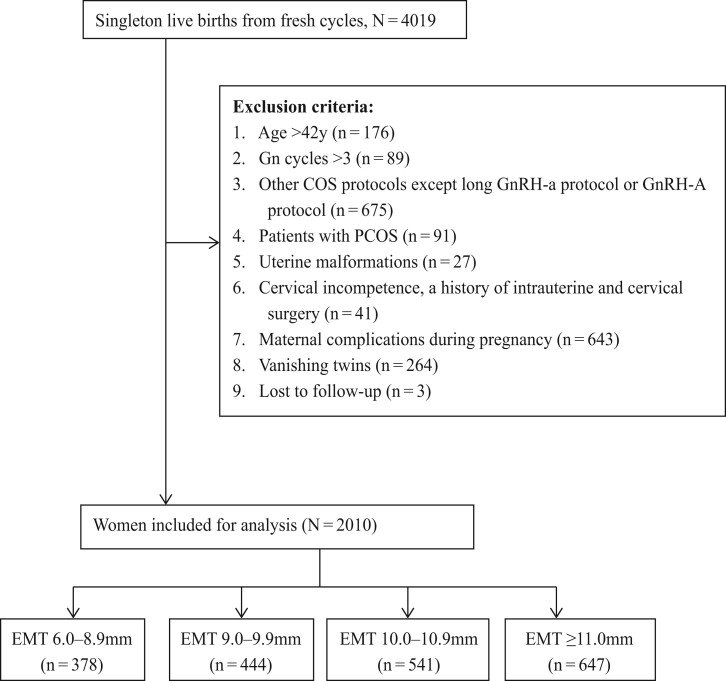
Study design size duration: This retrospective study involved singleton live births in women undergoing autologous IVF cycles during the period from 1 October 2016 to 31 July 2021.
Participants/materials setting methods: A total of 2010 women who fulfilled the inclusion criteria were included. A multivariable regression analysis was performed to detect the relationship between EMT and neonatal outcomes after controlling for potential confounders. Smooth curve fitting and threshold effect analysis were used to evaluate the accurate cutoff value of EMT.
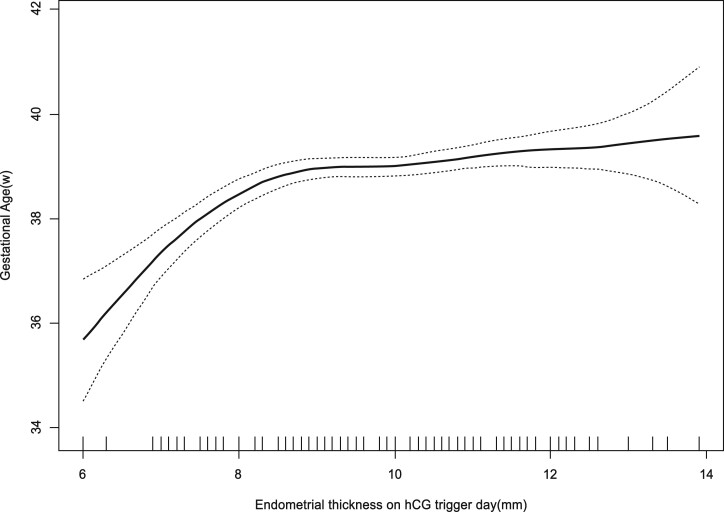
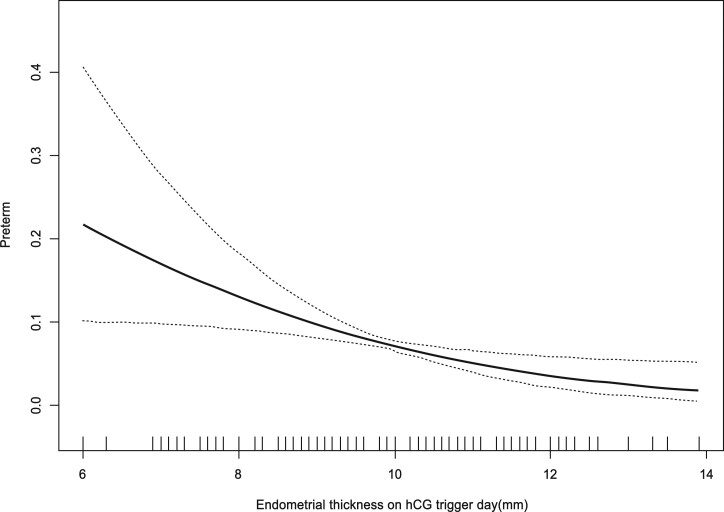
Main results and the role of chance: The results of the multivariate regression analyses showed that the odds of PTD were reduced by 45% with an EMT of 9.00-9.90 mm (adjusted odds ratio (OR): 0.55, 95% CI: 0.13 to 0.98; P = 0.0451), reduced by 58% with an EMT of 10.00-10.90 mm (adjusted OR: 0.42, 95% CI: 0.06 to 0.87; P = 0.0211) and reduced by 75% with an EMT >11 mm (adjusted OR: 0.25, 95% CI: 0.04 to 0.66; P = 0.0034), compared to the group with an EMT of 6.00-8.90 mm. It could also be seen from the adjusted smooth curves that the odds of PTD decreased and gestational age (GA) increased with increasing EMT. Combined with the analysis of threshold effects, the results indicated that when the EMT was ≤7.6 mm, the incidence of PTD decreased as the EMT gradually increased (adjusted OR: 0.47, 95% CI: 0.03 to 0.99; P = 0.0107), and when the EMT was ≤7.8 mm, the GA increased (adjusted β: 1.94, 95% CI: 1.26 to 2.63; P < 0.0001) as the EMT gradually increased.
Limitations reasons for caution: The main limitation of our study is its retrospective design. Although we found a significant decrease in PTD as the EMT increased, in terms of GA, the magnitude of the differences was modest, which may limit the clinical relevance of the findings.
Wider implications of the findings: Our data provide new insight into the relationship between EMT and neonatal outcomes by indicating that a thin endometrium of ≤7.8 mm is associated with an increased odds of PTD of singletons after fresh ET.
Study funding/competing interests: This study was supported by the National Natural Science Foundation of China (grant no. 82071717). There are no conflicts of interest.
Keywords: endometrial thickness (EMT); fresh embryo transfer; gestational age (GA); hCG trigger day; preterm delivery (PTD).
© The Author(s) 2023. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Brosens JJ, Pijnenborg R, Brosens IA.. The myometrial junctional zone spiral arteries in normal and abnormal pregnancies. a review of the literature. Am J Obstet Gynecol 2002;187:1416–1423. - PubMed
-
- Casper RF. It’s time to pay attention to the endometrium. Fertil Steril 2011;96:519–521. - PubMed
-
- Chung K, Coutifaris C, Chalian R, Lin K, Ratcliffe SJ, Castelbaum AJ, Freedman MF, Barnhart KT.. Factors influencing adverse perinatal outcomes in pregnancies achieved through use of in vitro fertilization. Fertil Steril 2006;86:1634–1641. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials