

Detection of Left Ventricular Systolic Dysfunction From Electrocardiographic Images
- PMID: 37489538
- PMCID: PMC10982757
- DOI: 10.1161/CIRCULATIONAHA.122.062646
Detection of Left Ventricular Systolic Dysfunction From Electrocardiographic Images
Abstract
Background: Left ventricular (LV) systolic dysfunction is associated with a >8-fold increased risk of heart failure and a 2-fold risk of premature death. The use of ECG signals in screening for LV systolic dysfunction is limited by their availability to clinicians. We developed a novel deep learning-based approach that can use ECG images for the screening of LV systolic dysfunction.
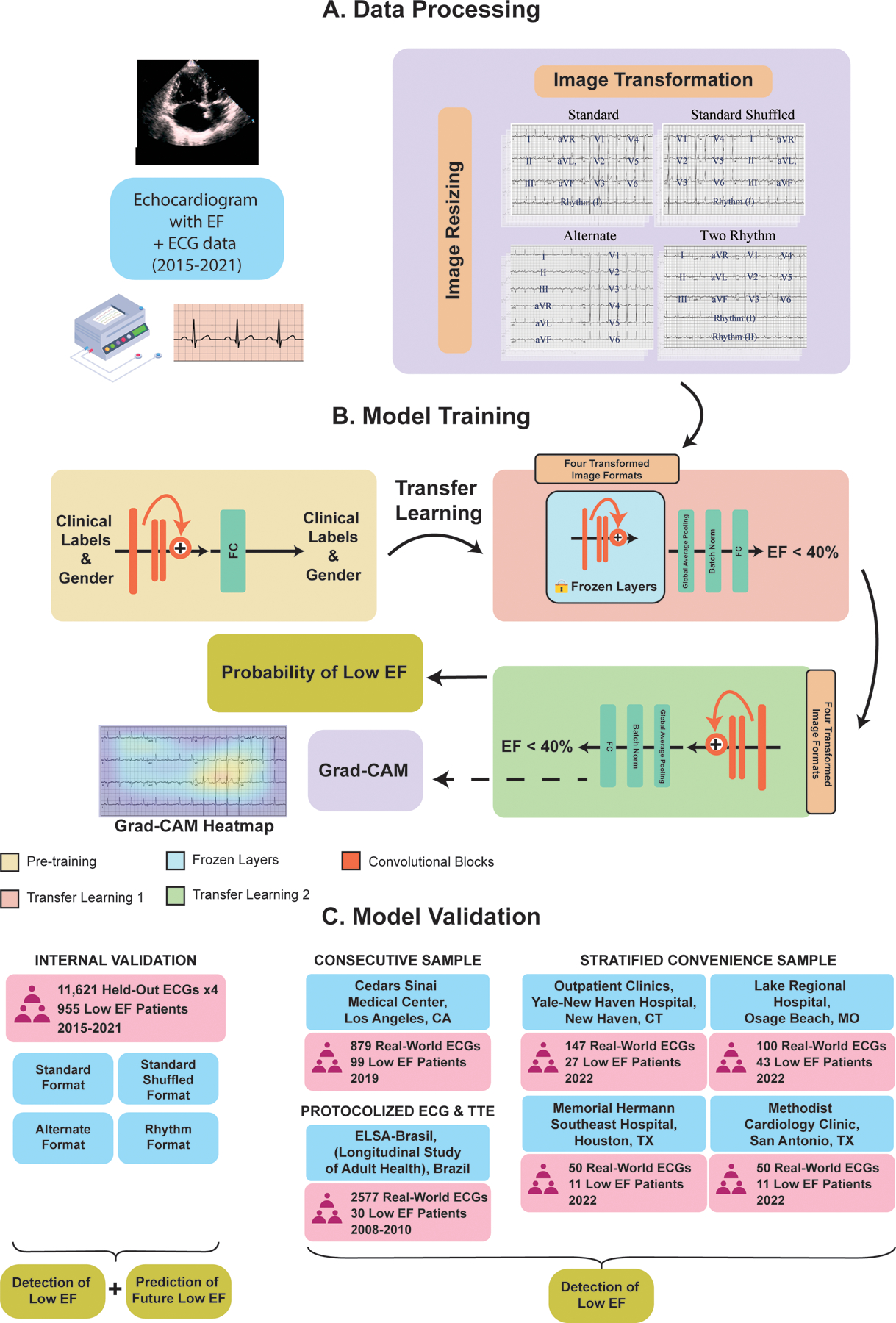
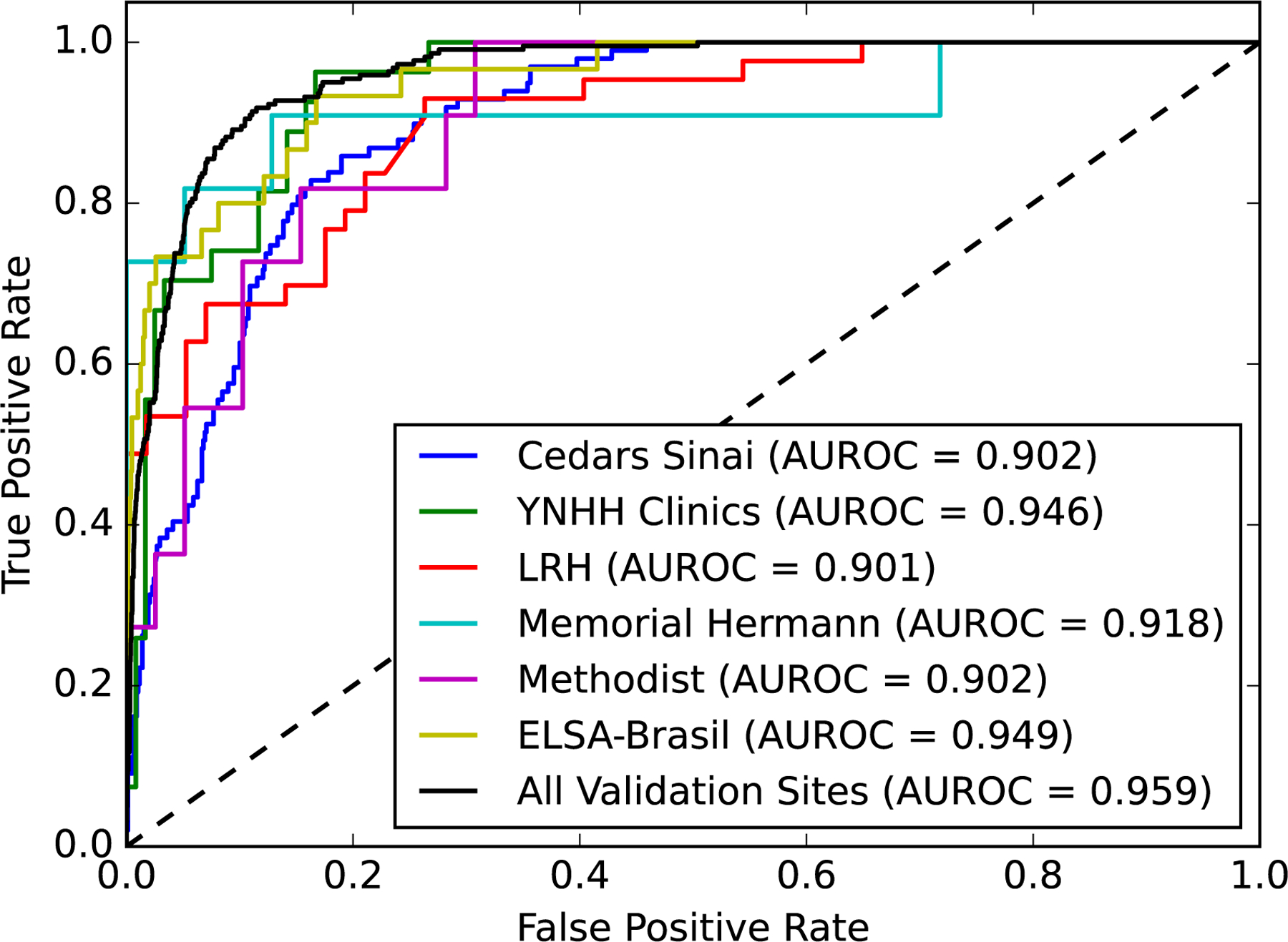
Methods: Using 12-lead ECGs plotted in multiple different formats, and corresponding echocardiographic data recorded within 15 days from the Yale New Haven Hospital between 2015 and 2021, we developed a convolutional neural network algorithm to detect an LV ejection fraction <40%. The model was validated within clinical settings at Yale New Haven Hospital and externally on ECG images from Cedars Sinai Medical Center in Los Angeles, CA; Lake Regional Hospital in Osage Beach, MO; Memorial Hermann Southeast Hospital in Houston, TX; and Methodist Cardiology Clinic of San Antonio, TX. In addition, it was validated in the prospective Brazilian Longitudinal Study of Adult Health. Gradient-weighted class activation mapping was used to localize class-discriminating signals on ECG images.
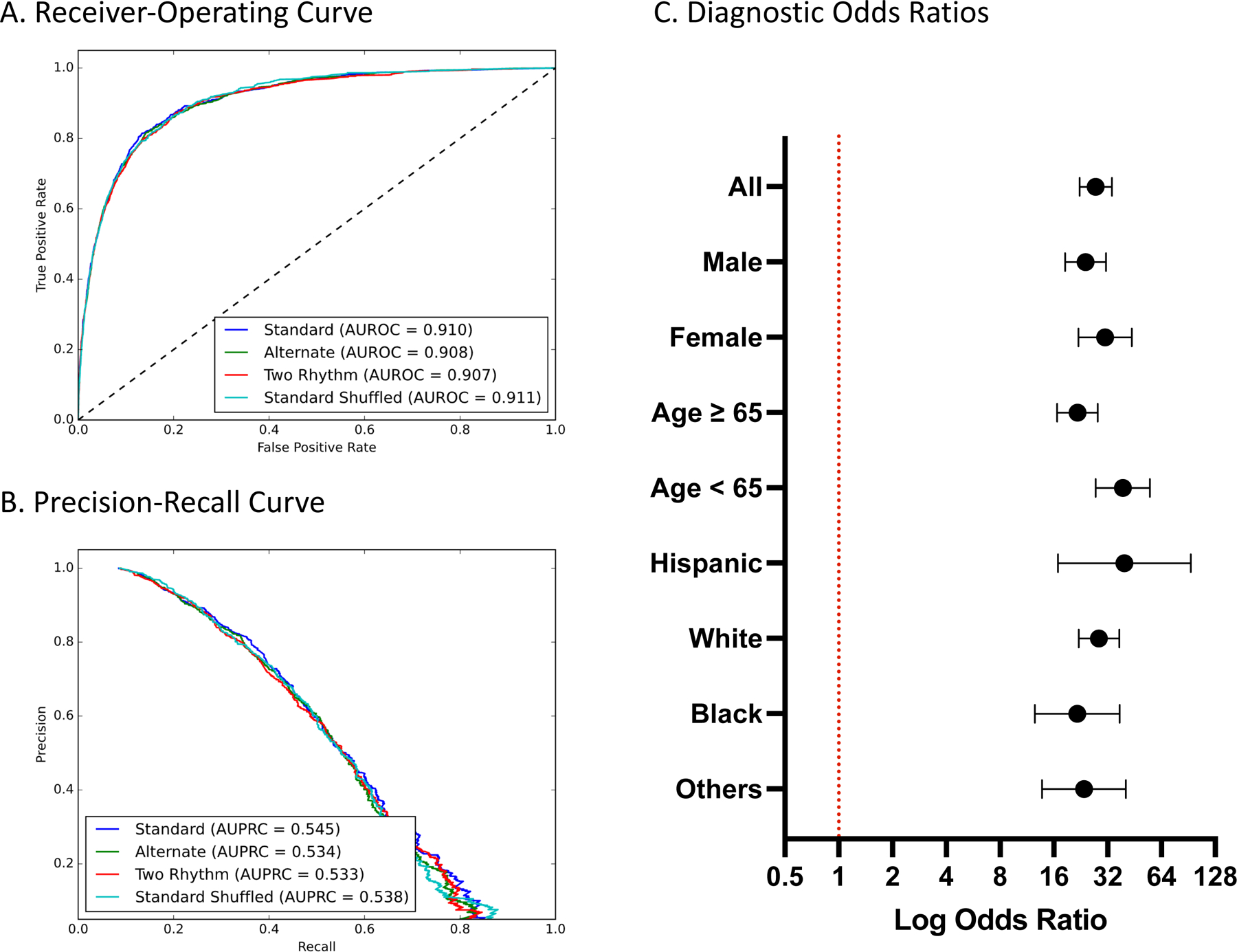
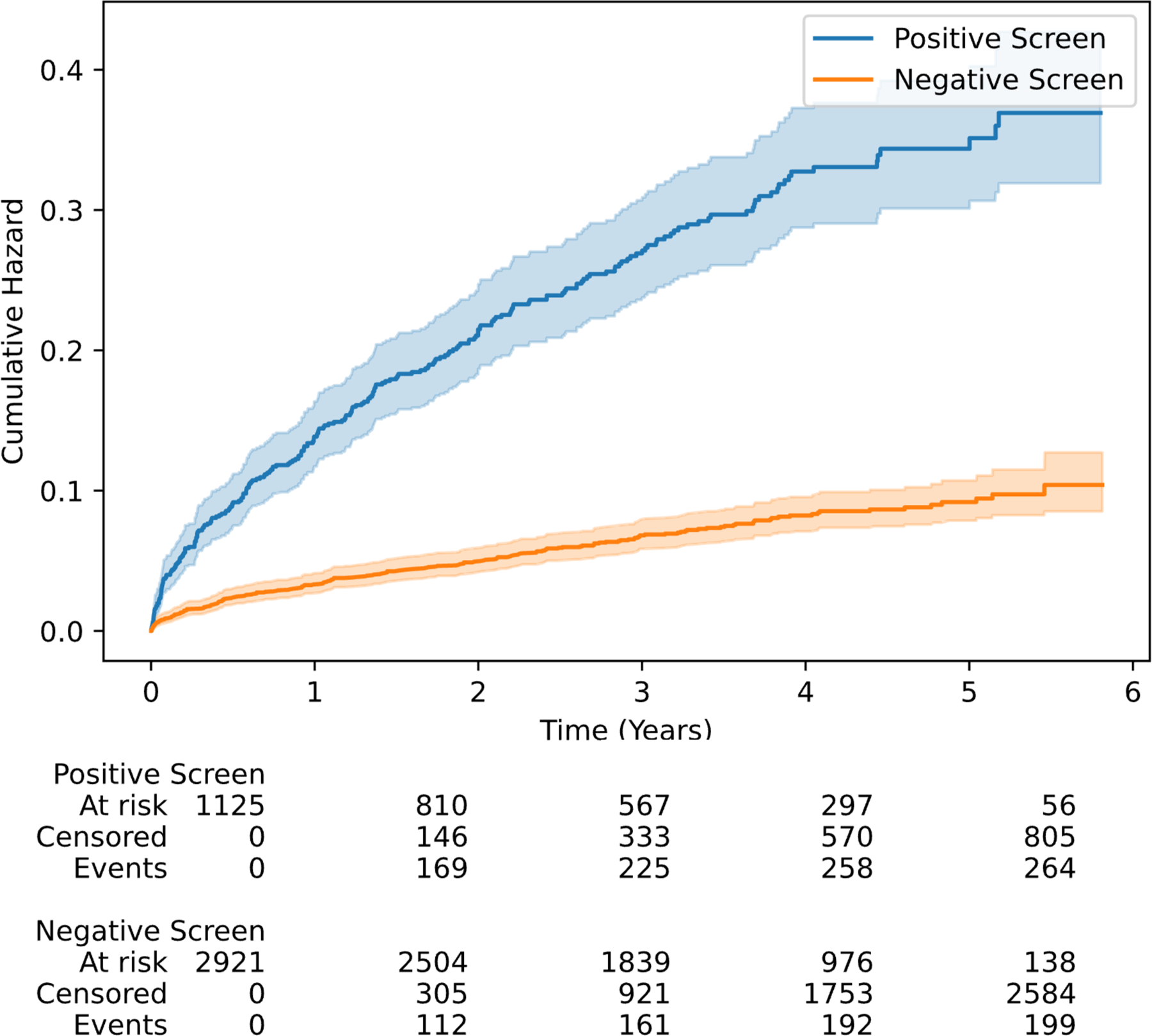
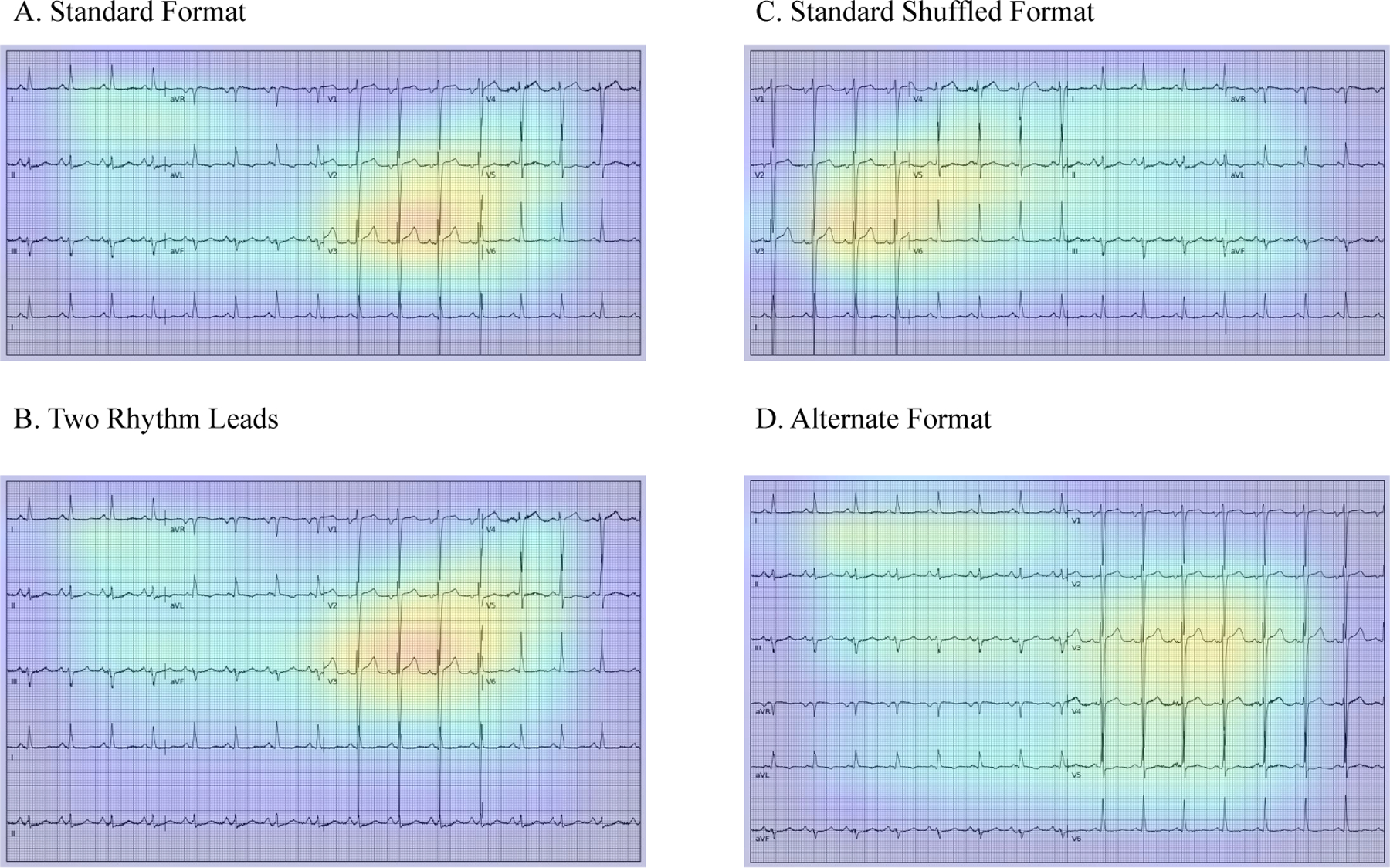
Results: Overall, 385 601 ECGs with paired echocardiograms were used for model development. The model demonstrated high discrimination across various ECG image formats and calibrations in internal validation (area under receiving operation characteristics [AUROCs], 0.91; area under precision-recall curve [AUPRC], 0.55); and external sets of ECG images from Cedars Sinai (AUROC, 0.90 and AUPRC, 0.53), outpatient Yale New Haven Hospital clinics (AUROC, 0.94 and AUPRC, 0.77), Lake Regional Hospital (AUROC, 0.90 and AUPRC, 0.88), Memorial Hermann Southeast Hospital (AUROC, 0.91 and AUPRC 0.88), Methodist Cardiology Clinic (AUROC, 0.90 and AUPRC, 0.74), and Brazilian Longitudinal Study of Adult Health cohort (AUROC, 0.95 and AUPRC, 0.45). An ECG suggestive of LV systolic dysfunction portended >27-fold higher odds of LV systolic dysfunction on transthoracic echocardiogram (odds ratio, 27.5 [95% CI, 22.3-33.9] in the held-out set). Class-discriminative patterns localized to the anterior and anteroseptal leads (V2 and V3), corresponding to the left ventricle regardless of the ECG layout. A positive ECG screen in individuals with an LV ejection fraction ≥40% at the time of initial assessment was associated with a 3.9-fold increased risk of developing incident LV systolic dysfunction in the future (hazard ratio, 3.9 [95% CI, 3.3-4.7]; median follow-up, 3.2 years).
Conclusions: We developed and externally validated a deep learning model that identifies LV systolic dysfunction from ECG images. This approach represents an automated and accessible screening strategy for LV systolic dysfunction, particularly in low-resource settings.
Keywords: artificial intelligence; biomedical technology; electrocardiography; heart failure; machine learning; ventricular dysfunction, left.
Conflict of interest statement
Figures
References
-
- Wang TJ, Evans JC, Benjamin EJ, Levy D, LeRoy EC, Vasan RS. Natural history of asymptomatic left ventricular systolic dysfunction in the community. Circulation. 2003;108:977–982. - PubMed
-
- Srivastava PK, DeVore AD, Hellkamp AS, Thomas L, Albert NM, Butler J, Patterson JH, Spertus JA, Williams FB, Duffy CI, Hernandez AF, Fonarow GC. Heart Failure Hospitalization and Guideline-Directed Prescribing Patterns Among Heart Failure With Reduced Ejection Fraction Patients. JACC Heart Fail. 2021;9:28–38. - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;101161CIR0000000000001063. - PubMed
-
- Wang TJ, Levy D, Benjamin EJ, Vasan RS. The epidemiology of “asymptomatic” left ventricular systolic dysfunction: implications for screening. Ann Intern Med 2003;138:907–916. - PubMed
