

AI Body Composition in Lung Cancer Screening: Added Value Beyond Lung Cancer Detection
- PMID: 37489991
- PMCID: PMC10374937
- DOI: 10.1148/radiol.222937
AI Body Composition in Lung Cancer Screening: Added Value Beyond Lung Cancer Detection
Abstract
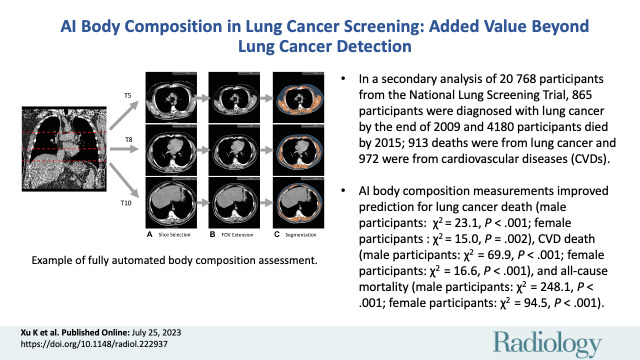
Background An artificial intelligence (AI) algorithm has been developed for fully automated body composition assessment of lung cancer screening noncontrast low-dose CT of the chest (LDCT) scans, but the utility of these measurements in disease risk prediction models has not been assessed. Purpose To evaluate the added value of CT-based AI-derived body composition measurements in risk prediction of lung cancer incidence, lung cancer death, cardiovascular disease (CVD) death, and all-cause mortality in the National Lung Screening Trial (NLST). Materials and Methods In this secondary analysis of the NLST, body composition measurements, including area and attenuation attributes of skeletal muscle and subcutaneous adipose tissue, were derived from baseline LDCT examinations by using a previously developed AI algorithm. The added value of these measurements was assessed with sex- and cause-specific Cox proportional hazards models with and without the AI-derived body composition measurements for predicting lung cancer incidence, lung cancer death, CVD death, and all-cause mortality. Models were adjusted for confounding variables including age; body mass index; quantitative emphysema; coronary artery calcification; history of diabetes, heart disease, hypertension, and stroke; and other PLCOM2012 lung cancer risk factors. Goodness-of-fit improvements were assessed with the likelihood ratio test. Results Among 20 768 included participants (median age, 61 years [IQR, 57-65 years]; 12 317 men), 865 were diagnosed with lung cancer and 4180 died during follow-up. Including the AI-derived body composition measurements improved risk prediction for lung cancer death (male participants: χ2 = 23.09, P < .001; female participants: χ2 = 15.04, P = .002), CVD death (males: χ2 = 69.94, P < .001; females: χ2 = 16.60, P < .001), and all-cause mortality (males: χ2 = 248.13, P < .001; females: χ2 = 94.54, P < .001), but not for lung cancer incidence (male participants: χ2 = 2.53, P = .11; female participants: χ2 = 1.73, P = .19). Conclusion The body composition measurements automatically derived from baseline low-dose CT examinations added predictive value for lung cancer death, CVD death, and all-cause death, but not for lung cancer incidence in the NLST. Clinical trial registration no. NCT00047385 © RSNA, 2023 Supplemental material is available for this article. See also the editorial by Fintelmann in this issue.
Conflict of interest statement
Figures





![Estimated unadjusted hazard ratios (HRs) of the lower and higher
groups, with the normal group as reference for each body composition
measurement (rows) and each end point event (columns) in male and female
participants. The groups were obtained by the stratification based on the
sex-specific 25th and 75th percentiles for each measurement. (A) Plot
displays the estimated unadjusted HRs in male participants (n =
12 317). (B) Plot displays the estimated unadjusted HRs in female
participants (n = 8451). The dots represent the estimated HRs. The segments
represent the 95% CIs of the estimated HRs. The HR of 1 (no difference in
hazard) is displayed as a red line in each plot for reference. The numbers
following each dot-segment combination show the numerical value of the HR,
with the 95% CI in parentheses and the associated P value in square
brackets. For instance, as indicated by the fourth row in the column
“CVD Death (n = 680)” in A, the lower skeletal muscle (SM)
attenuation group in male participants (<27.6 HU) was associated with
higher risk for cardiovascular disease (CVD) death (HR, 2.27 [95% CI: 1.93,
2.67]; P < .001) when compared with the normal group, which is
consistent with observations in Figure 4C based on cumulative incidence
functions. SAT = subcutaneous adipose tissue.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/c0aa/10374937/0113835b7f41/radiol.222937.fig6.jpg)
Comment in
-
Body Composition Analysis on Chest CT Scans: A Value Proposition for Lung Cancer Care.Radiology. 2023 Jul;308(1):e231205. doi: 10.1148/radiol.231205. Radiology. 2023. PMID: 37489985 No abstract available.
References
-
- Dulloo AG , Jacquet J , Solinas G , Montani JP , Schutz Y . Body composition phenotypes in pathways to obesity and the metabolic syndrome . Int J Obes 2010. ; 34 ( Suppl 2 ): S4 – S17 . - PubMed
-
- Eid AA , Ionescu AA , Nixon LS , et al. Inflammatory response and body composition in chronic obstructive pulmonary disease . Am J Respir Crit Care Med 2001. ; 164 ( 8 Pt 1 ): 1414 - 1418 . - PubMed
-
- Goodpaster BH , Park SW , Harris TB , et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study . J Gerontol A Biol Sci Med Sci 2006. ; 61 ( 10 ): 1059 – 1064 . - PubMed
-
- Troschel AS , Troschel FM , Best TD , et al. Computed tomography-based body composition analysis and its role in lung cancer care . J Thorac Imaging 2020. ; 35 ( 2 ): 91 – 100 . - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
