

Identifying Children Likely to Benefit From Antibiotics for Acute Sinusitis: A Randomized Clinical Trial
- PMID: 37490085
- PMCID: PMC10370259
- DOI: 10.1001/jama.2023.10854
Identifying Children Likely to Benefit From Antibiotics for Acute Sinusitis: A Randomized Clinical Trial
Erratum in
-
Removal of Conflict of Interest Disclosure.JAMA. 2024 Jul 9;332(2):173. doi: 10.1001/jama.2024.11869. JAMA. 2024. PMID: 38864163 Free PMC article. No abstract available.
Abstract
Importance: The large overlap between symptoms of acute sinusitis and viral upper respiratory tract infection suggests that certain subgroups of children being diagnosed with acute sinusitis, and subsequently treated with antibiotics, derive little benefit from antibiotic use.
Objective: To assess if antibiotic therapy could be appropriately withheld in prespecified subgroups.
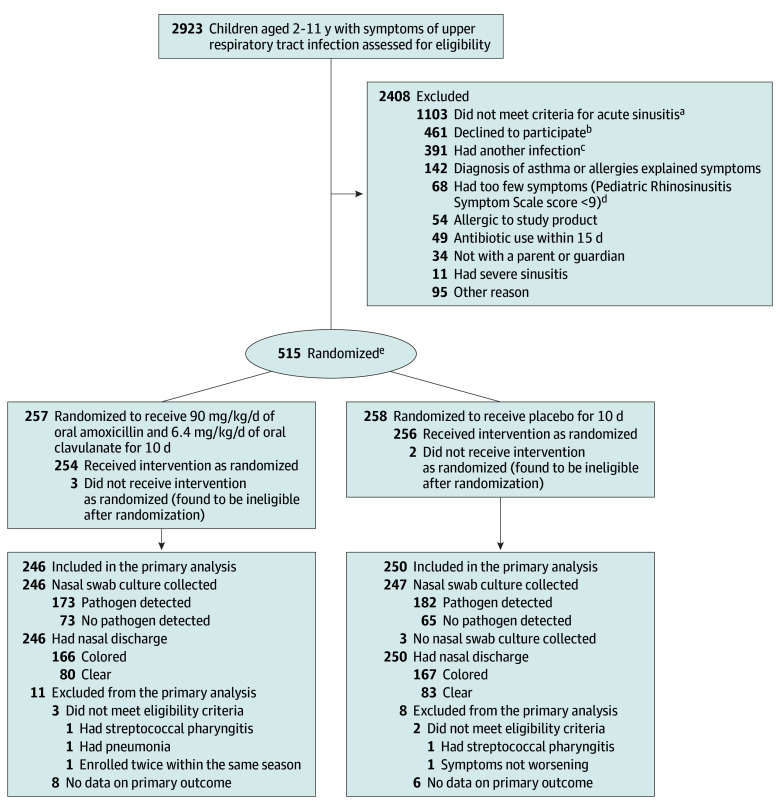
Design, setting, and participants: Randomized clinical trial including 515 children aged 2 to 11 years diagnosed with acute sinusitis based on clinical criteria. The trial was conducted between February 2016 and April 2022 at primary care offices affiliated with 6 US institutions and was designed to evaluate whether symptom burden differed in subgroups defined by nasopharyngeal Streptococcus pneumoniae, Haemophilus influenzae, or Moraxella catarrhalis on bacterial culture and by the presence of colored nasal discharge.
Interventions: Oral amoxicillin (90 mg/kg/d) and clavulanate (6.4 mg/kg/d) (n = 254) or placebo (n = 256) for 10 days.
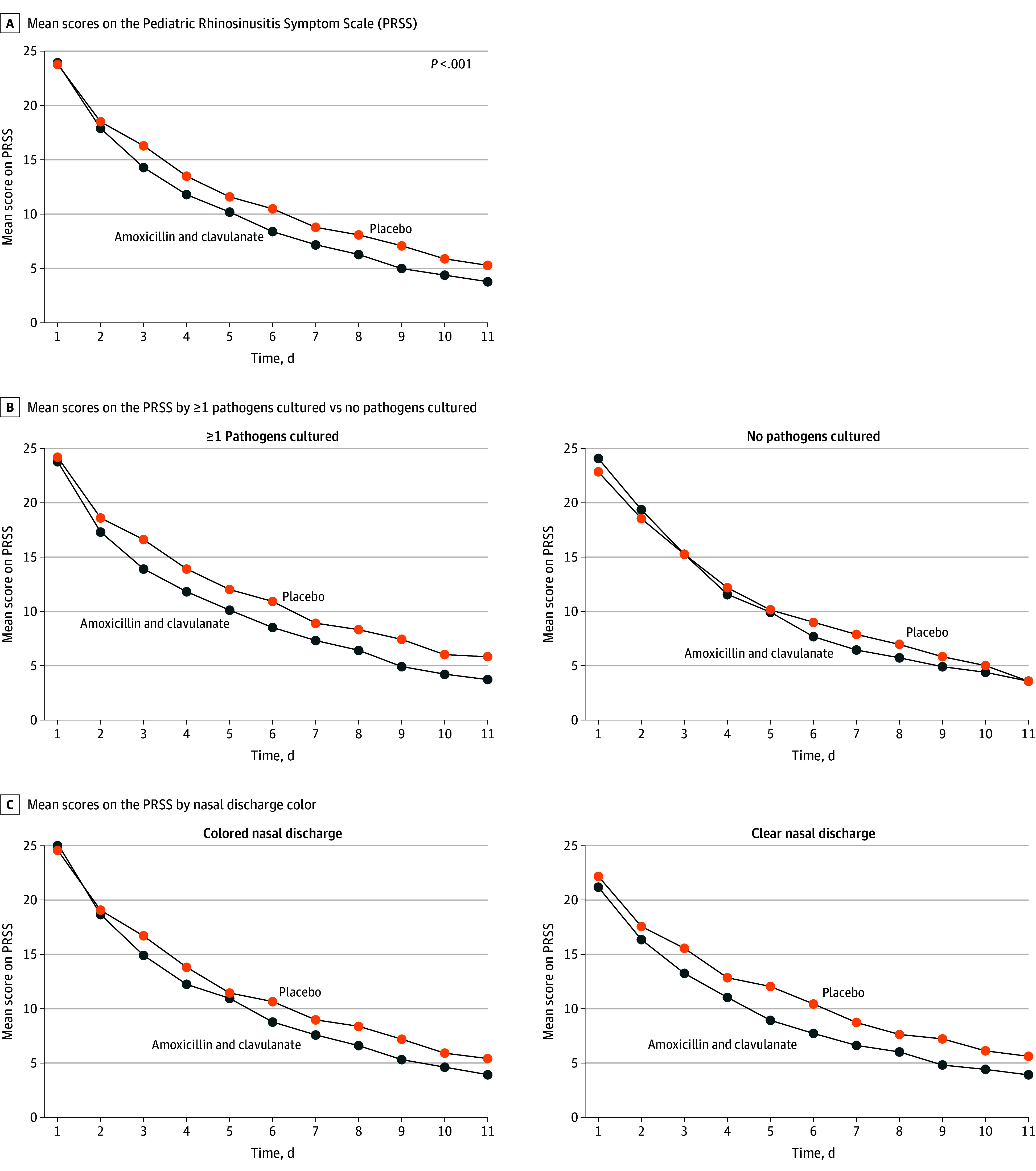
Main outcomes and measures: The primary outcome was symptom burden based on daily symptom scores on a validated scale (range, 0-40) during the 10 days after diagnosis. Secondary outcomes included treatment failure, adverse events including clinically significant diarrhea, and resource use by families.
Results: Most of the 510 included children were aged 2 to 5 years (64%), male (54%), White (52%), and not Hispanic (89%). The mean symptom scores were significantly lower in children in the amoxicillin and clavulanate group (9.04 [95% CI, 8.71 to 9.37]) compared with those in the placebo group (10.60 [95% CI, 10.27 to 10.93]) (between-group difference, -1.69 [95% CI, -2.07 to -1.31]). The length of time to symptom resolution was significantly lower for children in the antibiotic group (7.0 days) than in the placebo group (9.0 days) (P = .003). Children without nasopharyngeal pathogens detected did not benefit from antibiotic treatment as much as those with pathogens detected; the between-group difference in mean symptom scores was -0.88 (95% CI, -1.63 to -0.12) in those without pathogens detected compared with -1.95 (95% CI, -2.40 to -1.51) in those with pathogens detected. Efficacy did not differ significantly according to whether colored nasal discharge was present (the between-group difference was -1.62 [95% CI, -2.09 to -1.16] for colored nasal discharge vs -1.70 [95% CI, -2.38 to -1.03] for clear nasal discharge; P = .52 for the interaction between treatment group and the presence of colored nasal discharge).
Conclusions: In children with acute sinusitis, antibiotic treatment had minimal benefit for those without nasopharyngeal bacterial pathogens on presentation, and its effects did not depend on the color of nasal discharge. Testing for specific bacteria on presentation may represent a strategy to reduce antibiotic use in this condition.
Trial registration: ClinicalTrials.gov Identifier: NCT02554383.
Conflict of interest statement
Figures
Comment in
-
Acute Bacterial Sinusitis: Limitations of Test-Based Treatment.JAMA. 2023 Jul 25;330(4):326-327. doi: 10.1001/jama.2023.11365. JAMA. 2023. PMID: 37490097 No abstract available.
-
Antibiotics for Acute Sinusitis in Children.JAMA. 2023 Nov 21;330(19):1909-1910. doi: 10.1001/jama.2023.18833. JAMA. 2023. PMID: 37988098 No abstract available.
References
-
- Faden H, Stanievich J, Brodsky L, Bernstein J, Ogra PL. Changes in nasopharyngeal flora during otitis media of childhood. Pediatr Infect Dis J. 1990;9(9):623-626. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
