

Acute and mid-term outcomes of ablation for atrial fibrillation with VISITAG SURPOINT: the Japan MIYABI registry
- PMID: 37490850
- PMCID: PMC10492225
- DOI: 10.1093/europace/euad221
Acute and mid-term outcomes of ablation for atrial fibrillation with VISITAG SURPOINT: the Japan MIYABI registry
Erratum in
-
Correction to: Acute and mid-term outcomes of ablation for atrial fibrillation with VISITAG SURPOINT: the Japan MIYABI registry.Europace. 2025 Feb 5;27(2):euae261. doi: 10.1093/europace/euae261. Europace. 2025. PMID: 39937450 Free PMC article. No abstract available.
Abstract
Aims: The effectiveness of pulmonary vein isolation (PVI) guided by VISITAG SURPOINT (VS) has been demonstrated in Western populations. However, data for Asian populations are limited. VS settings may differ for Asians, given their smaller body size. This study aimed to describe outcomes of radiofrequency atrial fibrillation (AF) ablation guided by VS in a large Asian population.
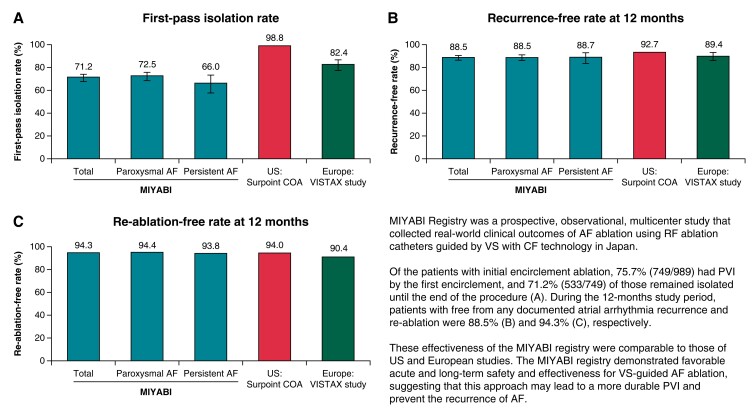
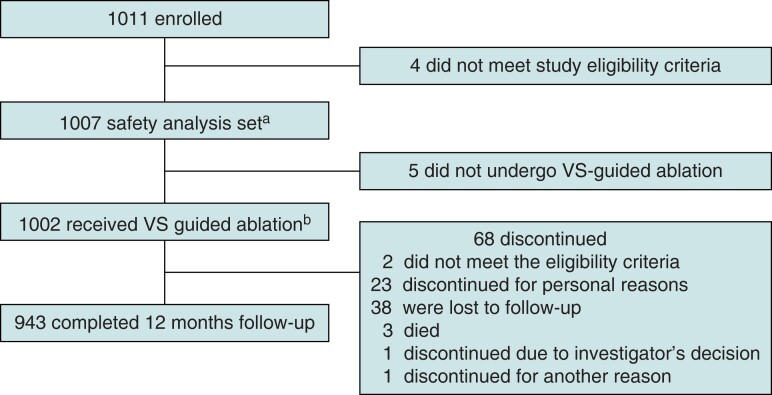
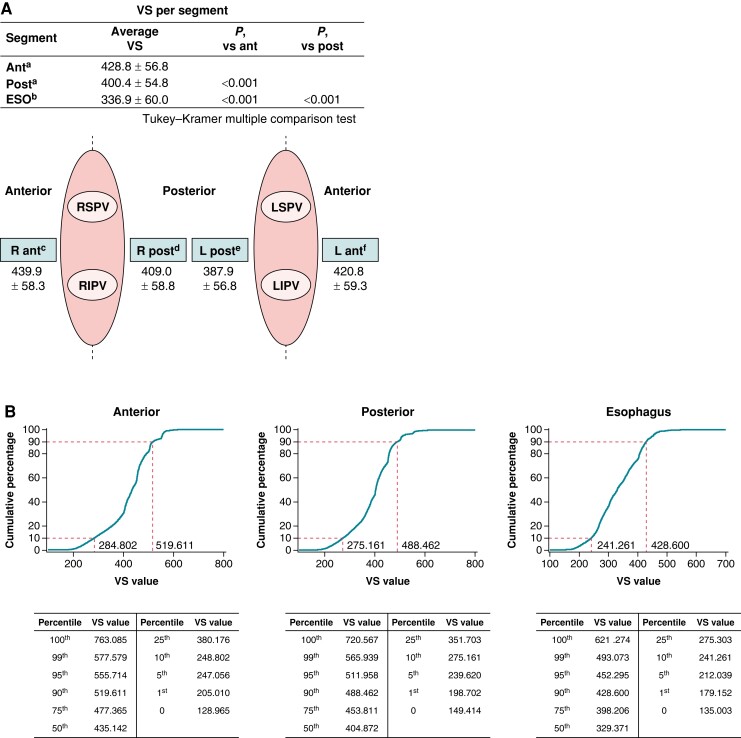
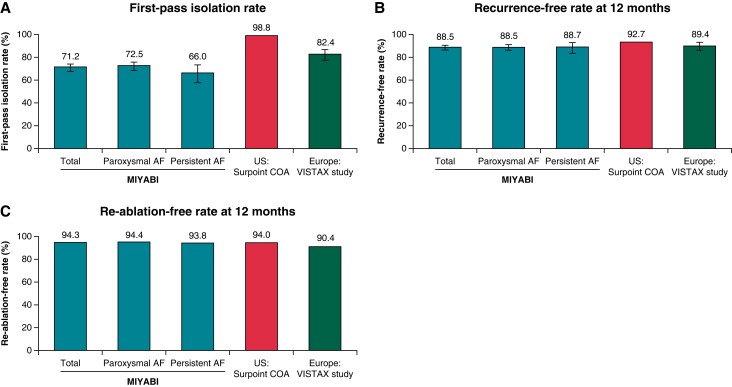
Methods and results: The prospective, observational, multicentre MIYABI registry collected real-world data from patients undergoing VS-guided AF ablation using ThermoCool SmartTouch and ThermoCool SmartTouch SF catheters from 50 Japanese centres. All patients had paroxysmal AF or persistent AF for <6 months. Primary adverse events (PAEs) were evaluated for safety. The primary efficacy endpoint was the proportion of patients with PVI at the end of the procedure. Mid-term effectiveness (up to 12 months) was evaluated by freedom from documented atrial arrhythmias. Of the 1011 patients enrolled, 1002 completed AF ablation. The mean number of VS values per procedure was 428.8 on the anterior wall and 400.4 on the posterior wall. Nine patients (0.9%) experienced PAEs. Upon procedure completion, 99.7% of patients had PVI. Twelve-month freedom from atrial arrhythmia recurrence was 88.5%; 5.7% of patients were re-ablated. At repeat ablation, 54% of RSPV, 73% of RIPV, 70% of LSPV, and 86% of LIPV evaluated remained durably isolated.
Conclusion: Despite lower anterior wall VS values compared with the CLOSE protocol (≥550), the present study demonstrated comparable efficacy outcomes, indicating that a VS of ≥550 for the anterior wall may not be necessary for Asian patients.
Keywords: Ablation index; Asian; Atrial fibrillation; Pulmonary vein isolation; VISITAG SURPOINT.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: K.O. received lecture fees from Johnson & Johnson K.K. as part of the submitted work and received lecture fees from Daiichi Sankyo Co., Ltd; Nippon Boehringer Ingelheim Co., Ltd; Bristol-Myers Squibb K.K.; and Medtronic Japan Co., Ltd outside of the submitted work. K.I. received remuneration for lecture, consultant, and proctor from Johnson & Johnson K.K. as part of the submitted work and received remuneration for lecture, consultant, and proctor from Medtronic Japan Co., Ltd; Boston Scientific Japan K.K.; Japan Lifeline Co., Ltd; Daiichi Sankyo Co., Ltd; Bayer Yakuhin, Ltd; Bristol-Myers Squibb K.K.; Nippon Boehringer Ingelheim Co., Ltd; and Abbott outside of the submitted work. M.G. received lecture fees from Johnson & Johnson K.K. as part of the submitted work and received lecture fees from Medtronic Japan Co., Ltd; Bayer Yakuhin, Ltd; Abbott, Phillips Japan, Ltd; Cook Medical Japan G.K.; and Japan Lifeline Co., Ltd, and received research funds from Japan Lifeline Co., Ltd, outside of the submitted work. H.O. received remuneration from Johnson & Johnson K.K. as part of the submitted work and received a writing fee from MSD K.K., a lecture fee from Canon Medial Systems Corp., and a consultant fee from Kaken Pharmaceutical Co., Ltd, outside of the submitted work. M.Y. is an employee of Johnson & Johnson K.K., as indicated in the submitted work. A.N. received honoraria from Biosense Webster, Inc., as part of the submitted work and received honoraria from Abbott and Biosense Webster, Inc., and an endowment from Medtronic Japan Co., Ltd, and DVx Inc. outside of the submitted work.
Figures
Comment in
-
Pulmonary vein isolation with composite index tagging: are we making ablation simpler or simple?Europace. 2023 Aug 2;25(9):euad259. doi: 10.1093/europace/euad259. Europace. 2023. PMID: 37656987 Free PMC article. No abstract available.
References
-
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SAet al. . 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace 2012;14:528–606. - PubMed
-
- Neuzil P, Reddy VY, Kautzner J, Petru J, Wichterle D, Shah Det al. . Electrical reconnection after pulmonary vein isolation is contingent on contact force during initial treatment: results from the EFFICAS I study. Circ Arrhythm Electrophysiol 2013;6:327–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
