

Enhanced detection of severe aortic stenosis via artificial intelligence: a clinical cohort study
- PMID: 37491129
- PMCID: PMC10373677
- DOI: 10.1136/openhrt-2023-002265
Enhanced detection of severe aortic stenosis via artificial intelligence: a clinical cohort study
Abstract
Objective: We developed an artificial intelligence decision support algorithm (AI-DSA) that uses routine echocardiographic measurements to identify severe aortic stenosis (AS) phenotypes associated with high mortality.
Methods: 631 824 individuals with 1.08 million echocardiograms were randomly spilt into two groups. Data from 442 276 individuals (70%) entered a Mixture Density Network (MDN) model to train an AI-DSA to predict an aortic valve area <1 cm2, excluding all left ventricular outflow tract velocity or dimension measurements and then using the remainder of echocardiographic measurement data. The optimal probability threshold for severe AS detection was identified at the f1 score probability of 0.235. An automated feature also ensured detection of guideline-defined severe AS. The AI-DSA's performance was independently evaluated in 184 301 (30%) individuals.
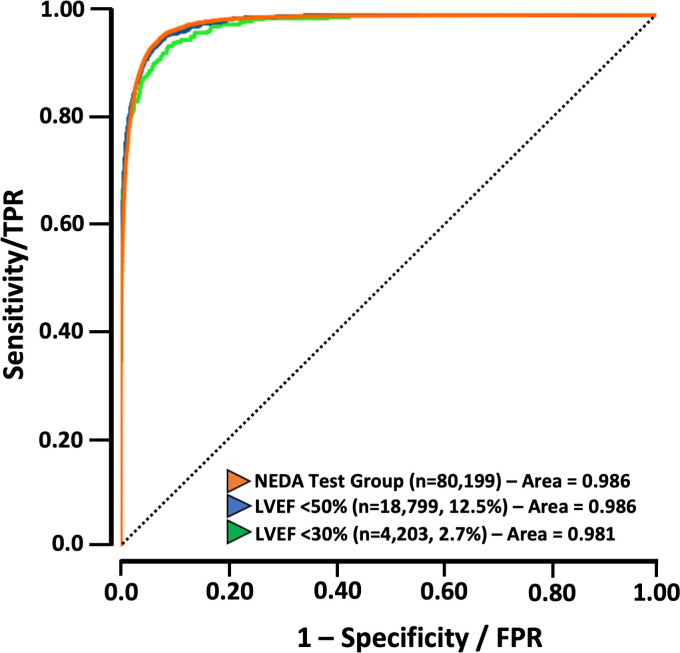
Results: The area under receiver operating characteristic curve for the AI-DSA to detect severe AS was 0.986 (95% CI 0.985 to 0.987) with 4622/88 199 (5.2%) individuals (79.0±11.9 years, 52.4% women) categorised as 'high-probability' severe AS. Of these, 3566 (77.2%) met guideline-defined severe AS. Compared with the AI-derived low-probability AS group (19.2% mortality), the age-adjusted and sex-adjusted OR for actual 5-year mortality was 2.41 (95% CI 2.13 to 2.73) in the high probability AS group (67.9% mortality)-5-year mortality being slightly higher in those with guideline-defined severe AS (69.1% vs 64.4%; age-adjusted and sex-adjusted OR 1.26 (95% CI 1.04 to 1.53), p=0.021).
Conclusions: An AI-DSA can identify the echocardiographic measurement characteristics of AS associated with poor survival (with not all cases guideline defined). Deployment of this tool in routine clinical practice could improve expedited identification of severe AS cases and more timely referral for therapy.
Keywords: Aortic Valve Stenosis; Echocardiography; Translational Medical Research.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Profs Stewart, Playford and Strange have previously received consultancy/speaking fees from Edwards Lifesciences. Profs Playford and Strange have received consultancy fees from Medtronic, Edwards Lifesciences, Abbott Laboratories and ECHO IQ Pty Ltd. Dr Watts is employed by ECHO IQ Pty Ltd.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous