

Factors associated with alteration of nipple or skin sensation and impact of duration of time following nipple-sparing mastectomy (NSM): an analysis of 460 cases with comparison of conventional versus endoscopic- or robotic-assisted NSM
- PMID: 37491239
- PMCID: PMC10369824
- DOI: 10.1186/s12957-023-03107-5
Factors associated with alteration of nipple or skin sensation and impact of duration of time following nipple-sparing mastectomy (NSM): an analysis of 460 cases with comparison of conventional versus endoscopic- or robotic-assisted NSM
Abstract
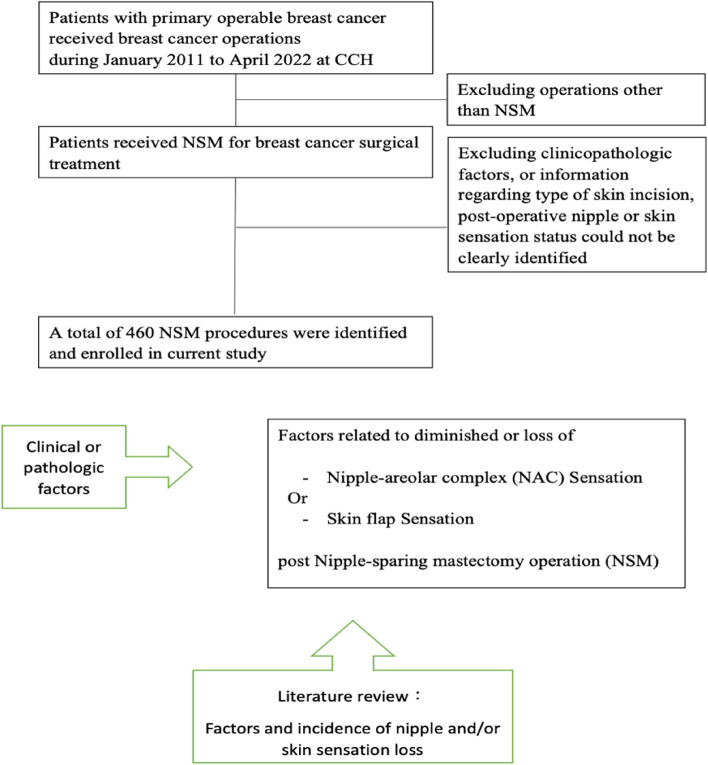
Background: The current study aims to evaluate the nipple and skin sensation following nipple-sparing mastectomy (NSM) and identify patient-, surgical-, or treatment-related factors affecting nipple or skin sensation in this cohort.
Methods: Patients who received NSM with postoperative nipple and skin sensation test evaluation at a single institution over the past 10 years were retrospectively retrieved from a prospectively collected breast cancer surgery database.
Results: A total of 460 NSM procedures were included in this current study, with the mean age of 48.3 ± 9.1. Three-hundred eighty-three (83.3%) patients had breast reconstructions. One-hundred seventy-four (37.8%) received conventional NSM (C-NSM), 195 (42.4%) endoscopic-assisted NSM (E-NSM), and 91 (19.8%) robotic-assisted NSM (R-NSM) procedures. For nipple sensation assessment, 15 (3.3%) were grade 0, 83 (18.2%) grade I, 229 (49.7%) grade II, and 133 (28.9%) grade III (normal sensation), respectively, with mean grade score of 2.1 ± 0.7. The preserved (grade III) nipple sensation rate was 36.2% (63/174) in the C-NSM group, 26.7% (52/195) in the E-NSM group, and 19.7% (18/91) in the R-NSM group (P = 0.06). The "time since surgery to last evaluation" was significantly longer in the C-NSM group (45.6 ± 34 months) or E-NSM group (44.7 ± 35.8 months) as compared to R-NSM group (31.8 ± 16 months, P < 0.01). In multivariate analysis, peri-areolar incision showed higher grade of nipple sensation (OR: 2.1, P = 0.02) compared to upper outer quadrant incision, and longer follow-up time post-NSM showed significant improvement of nipple or skin sensation (> 60 months vs. ≦ 12 months: nipple odds ratio (OR) = 5.75, P < 0.01; skin, OR = 1.97, P < 0.05).
Conclusion: Our current analysis showed some factors to be related to postoperative nipple or skin sensation, and longer "time after surgery" was associated with significant improvement of nipple and skin sensation in patients who received NSM, regardless of the surgical approaches.
Synopsis: Our current analysis showed a significant portion of patients with decrease or loss of nipple or skin sensation after nipple-sparing mastectomy (NSM). Several factors associated with preserved nipple or skin sensation were identified, including age, surgical methods, surgical wound location, and association of time from surgery showing that improvement of partial nipple or skin sensation was evident after a longer follow-up.
Keywords: Breast cancer; Conventional nipple-sparing mastectomy (C-NSM); Endoscopic-assisted nipple-sparing mastectomy (E-NSM); Nipple areola complex (NAC); Nipple sensation; Nipple-sparing mastectomy (NSM); Robotic-assisted nipple-sparing mastectomy (R-NSM); Skin sensation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
