

Bortezomib, lenalidomide and dexamethasone (VRd) vs carfilzomib, lenalidomide and dexamethasone (KRd) as induction therapy in newly diagnosed multiple myeloma
- PMID: 37491332
- PMCID: PMC10368661
- DOI: 10.1038/s41408-023-00882-y
Bortezomib, lenalidomide and dexamethasone (VRd) vs carfilzomib, lenalidomide and dexamethasone (KRd) as induction therapy in newly diagnosed multiple myeloma
Abstract
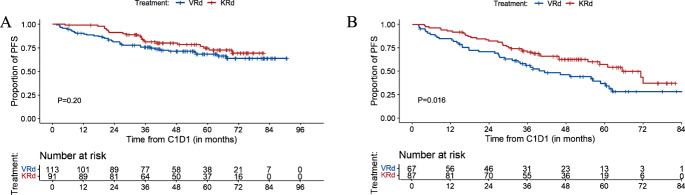
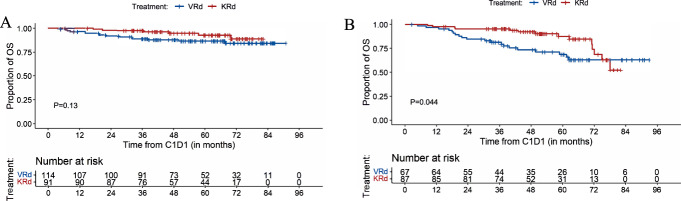
Lenalidomide and dexamethasone with bortezomib (VRd) or carfilzomib (KRd) are commonly used induction regimens in the U.S. This single-center, retrospective study evaluated outcomes and safety of VRd and KRd. Primary endpoint was progression-free survival (PFS). Of 389 patients with newly diagnosed multiple myeloma, 198 received VRd and 191 received KRd. Median PFS was not reached (NR) in both groups; 5-year PFS was 56% (95%CI, 48-64%) for VRd and 67% (60-75%) for KRd (P = 0.027). Estimated 5-year EFS was 34% (95%CI, 27-42%) for VRd and 52% (45-60%) for KRd (P < 0.001) with corresponding 5-year OS of 80% (95%CI, 75-87%) and 90% (85-95%), respectively (P = 0.053). For standard-risk patients, 5-year PFS was 68% (95%CI, 60-78%) for VRd and 75% (65-85%) for KRd (P = 0.20) with 5-year OS of 87% (95%CI, 81-94%) and 93% (87-99%), respectively (P = 0.13). For high-risk patients, median PFS was 41 months (95%CI, 32.8-61.1) for VRd and 70.9 months (58.2-NR) for KRd (P = 0.016). Respective 5-year PFS and OS were 35% (95%CI, 24-51%) and 69% (58-82%) for VRd and 58% (47-71%) and 88% (80-97%, P = 0.044) for KRd. Overall, KRd resulted in improved PFS and EFS with a trend toward improved OS compared to VRd with associations primarily driven by improvements in outcome for high-risk patients.
© 2023. The Author(s).
Conflict of interest statement
CT reports research funding from Janssen and Takeda and personal fees from MJH Life Sciences; has participated in advisory boards for Janssen and Sanofi, outside of the submitted work. BD reports honoraria received from Janssen and Sanofi, outside the submitted work. MH reports research funding from Amgen, Daiichi Sankyo, GlaxoSmithKline; and has received honoraria for consultancy/participated in advisory boards for Curio Science LLC, Intellisphere LLC, Bristol Myer Squibb, and GlaxoSmithKline. HH reports grants from Celgene, Takeda, and Janssen, outside the submitted work. SM reports consulting fees from Evicore, Optum, BioAscend, Janssen Oncology and Legend Biotech. Memorial Sloan Kettering Cancer Center receives research funding from the NCI, Janssen Oncology, Bristol Myers Squibb, Allogene Therapeutics, Fate Therapeutics and Takeda Oncology for conducting research. SM received honoraria from OncLive, Physician Education Resource, MJH Life Sciences and Plexus Communications, outside the submitted work. US reports research funding from Celgene/Bristol Myers Squibb and Janssen; personal fees from Janssen, Sanofi, Bristol Myers Squibb; and honoraria for continuing medical education activity from MJH Life Sciences, MashUpMD, and ACCC, outside the submitted work. KM reports grant support from ASH, MMRF, and IMS. OBL reports serving on an advisory board for MorphoSys Inc and Kite. HJL reports research funding from Alexion Pharmaceuticals, Takeda, Janssen, Prothena, and Protego; and has received honoraria for consultancy/participated in advisory boards for Karyopharm, Pfizer, Juno, Prothena, Caelum Biosciences, Legend Biotech, Takeda, Janssen, and Nexcella. GLS reports research funding from Janssen, Amgen, BMS, Beyond Spring, and serves on the Data Safety Monitoring Board for ArcellX. MS served as a paid consultant for McKinsey & Company, Angiocrine Bioscience, Inc., and Omeros Corporation; received research funding from Angiocrine Bioscience, Inc., Omeros Corporation, and Amgen, Inc.; served on ad hoc advisory boards for Kite – A Gilead Company; and received honoraria from i3Health, Medscape, and CancerNetwork for CME-related activity. SAG reports personal fees and advisory role (scientific advisory board) from Actinium, Celgene, Bristol Myers Squibb, Sanofi, Amgen, Pfizer, GlaxoSmithKline, JAZZ, Janssen, Omeros, Takeda, and Kite, outside the submitted work. AL reports grants from Bristol Myers Squibb; grants, personal fees and non-financial support from Pfizer; and grants and personal fees from Janssen, outside the submitted work. AL serves on the Data Safety Monitoring Board for ArcellX and also has a patent US20150037346A1 with royalties paid. SZU received research funding from Amgen, Array Biopharma, BMS, Celgene, GSK, Janssen, Merck, Pharmacyclics, Sanofi, Seattle Genetics, SkylineDX, and Takeda, is a Consultant to Abbvie, Amgen, BMS, Celgene, EdoPharma, Genentech, Gilead, GSK, Janssen, Oncopeptides, Sanofi, Seattle Genetics, SecuraBio, SkylineDX, Takeda, TeneoBio, and is also a Speaker with Amgen, BMS, Janssen, Sanofi. OL has received grant support from LLS, Rising Tide Foundation, NIH, FDA, MMRF, IMF, Perelman Family Foundation, Amgen, Celgene, Janssen, Takeda, Glenmark, Seattle Genetics, Karyopharm; has received honoraria for scientific talks/participated in advisory boards for Adaptive, Amgen, Binding Site, BMS, Celgene, Cellectis, Glenmark, Janssen, Juno, Pfizer; and served on Independent Data Monitoring Committees (IDMC) for international randomized trials by Takeda, Merck, Janssen, Theradex. NK reports research funding through Amgen, Janssen, Epizyme, AbbVie; consults for CCO, OncLive, and Intellisphere Remedy Health; and participated in advisory board for Janssen.
Figures

Update of
-
Bortezomib, Lenalidomide and Dexamethasone (VRd) vs Carfilzomib, Lenalidomide and Dexamethasone (KRd) as Induction Therapy in Newly Diagnosed Multiple Myeloma.Res Sq [Preprint]. 2023 Feb 24:rs.3.rs-2583053. doi: 10.21203/rs.3.rs-2583053/v1. Res Sq. 2023. Update in: Blood Cancer J. 2023 Jul 25;13(1):112. doi: 10.1038/s41408-023-00882-y. PMID: 36865246 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
