

Safety and anti-tumour activity of the IgE antibody MOv18 in patients with advanced solid tumours expressing folate receptor-alpha: a phase I trial
- PMID: 37491373
- PMCID: PMC10368744
- DOI: 10.1038/s41467-023-39679-9
Safety and anti-tumour activity of the IgE antibody MOv18 in patients with advanced solid tumours expressing folate receptor-alpha: a phase I trial
Abstract
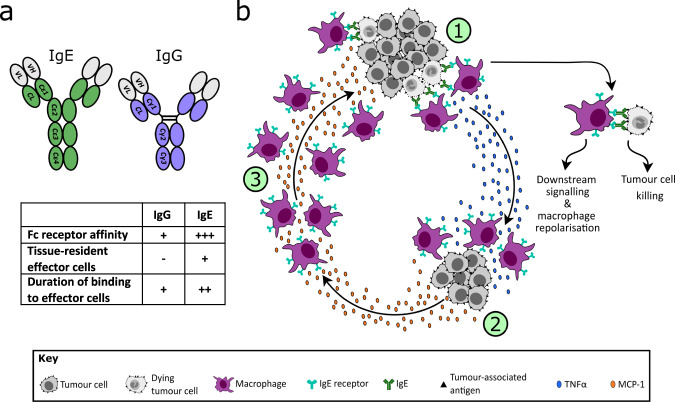
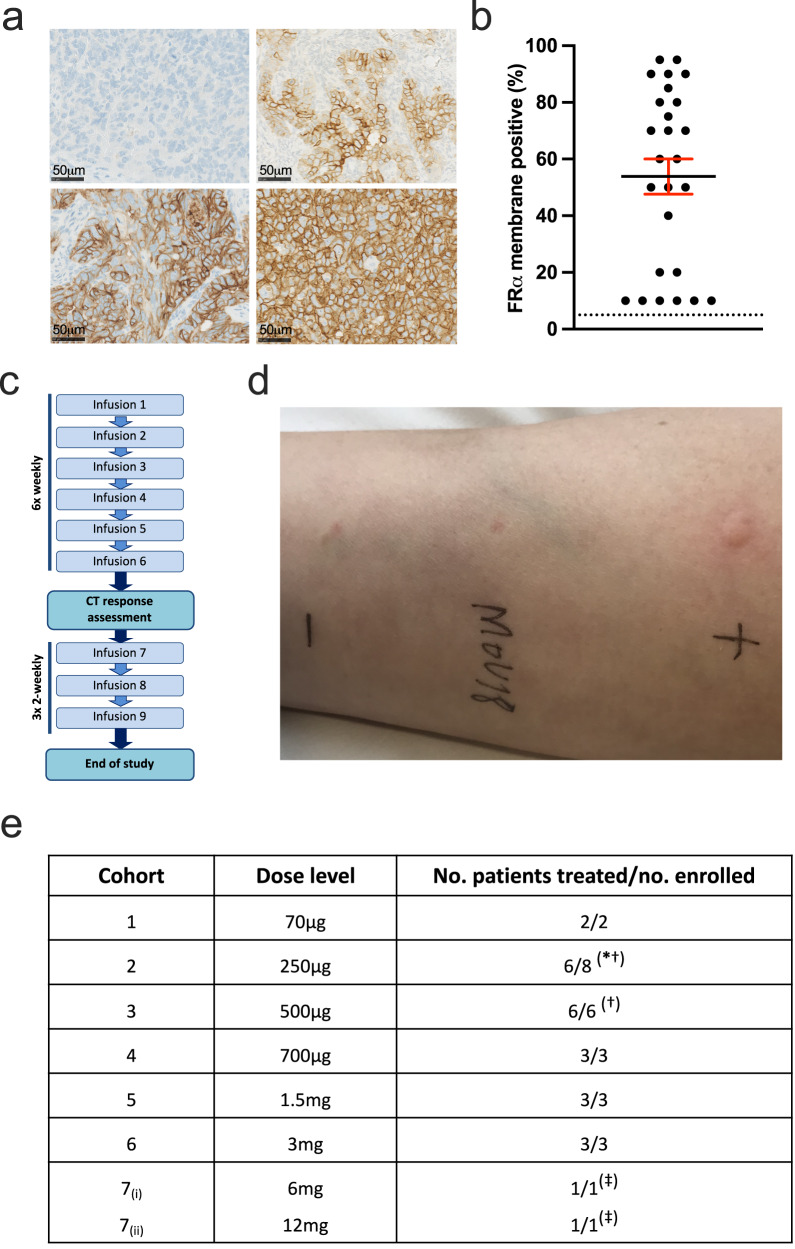
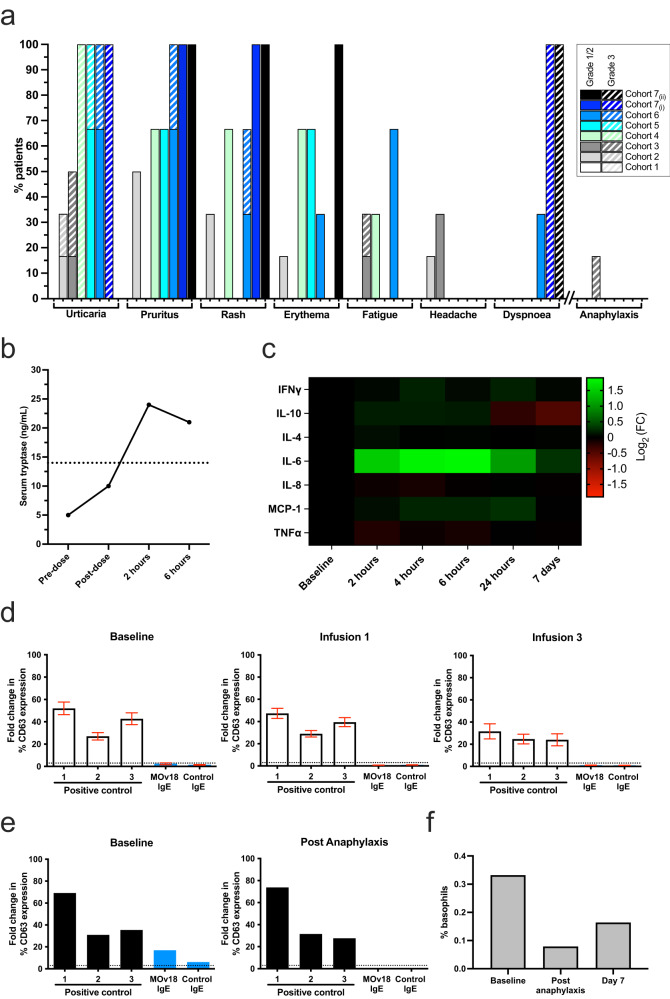
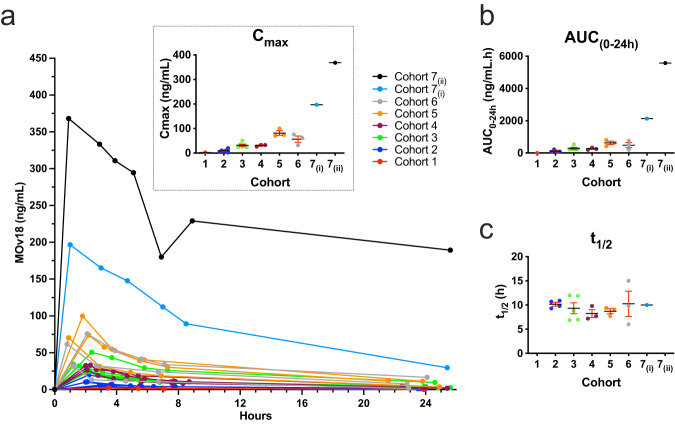
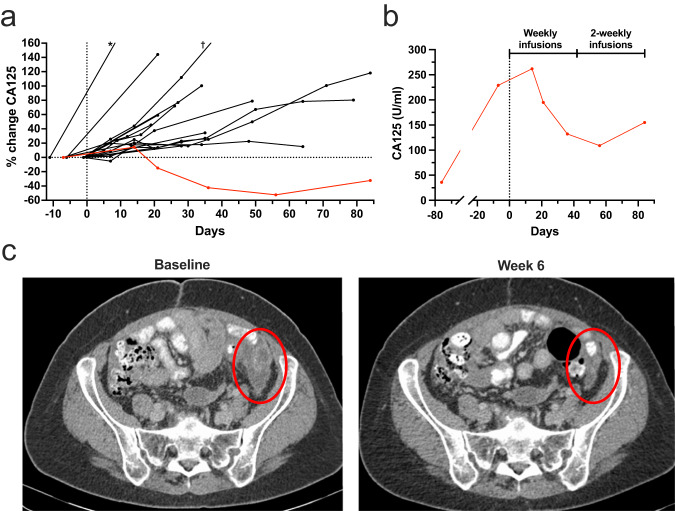
All antibodies approved for cancer therapy are monoclonal IgGs but the biology of IgE, supported by comparative preclinical data, offers the potential for enhanced effector cell potency. Here we report a Phase I dose escalation trial (NCT02546921) with the primary objective of exploring the safety and tolerability of MOv18 IgE, a chimeric first-in-class IgE antibody, in patients with tumours expressing the relevant antigen, folate receptor-alpha. The trial incorporated skin prick and basophil activation tests (BAT) to select patients at lowest risk of allergic toxicity. Secondary objectives were exploration of anti-tumour activity, recommended Phase II dose, and pharmacokinetics. Dose escalation ranged from 70 μg-12 mg. The most common toxicity of MOv18 IgE is transient urticaria. A single patient experienced anaphylaxis, likely explained by detection of circulating basophils at baseline that could be activated by MOv18 IgE. The BAT assay was used to avoid enrolling further patients with reactive basophils. The safety profile is tolerable and maximum tolerated dose has not been reached, with evidence of anti-tumour activity observed in a patient with ovarian cancer. These results demonstrate the potential of IgE therapy for cancer.
© 2023. The Author(s).
Conflict of interest statement
J.S. and S.K. are co-founders of Epsilogen Ltd. H.B. is presently employed, and J.C. formerly employed, through a fund from Epsilogen Ltd. S.K., H.B., H.G., D.J, G.P. and J.S. hold patents on anti-tumour IgE antibodies. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
