

A population-scale temporal case-control evaluation of COVID-19 disease phenotype and related outcome rates in patients with cancer in England (UKCCP)
- PMID: 37491478
- PMCID: PMC10368624
- DOI: 10.1038/s41598-023-36990-9
A population-scale temporal case-control evaluation of COVID-19 disease phenotype and related outcome rates in patients with cancer in England (UKCCP)
Abstract
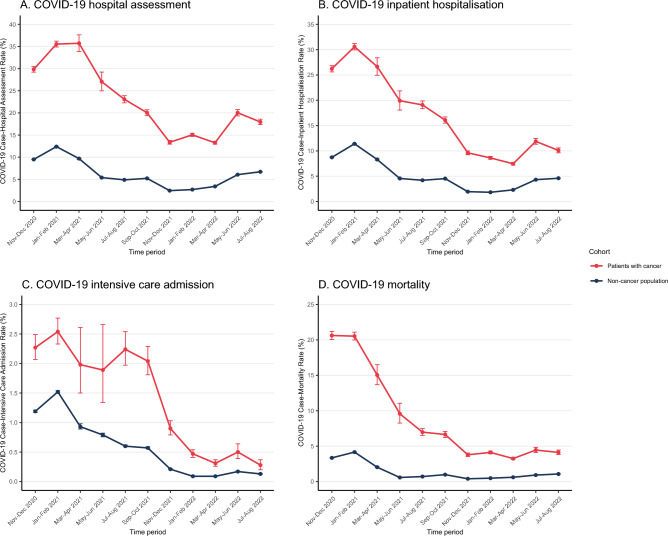
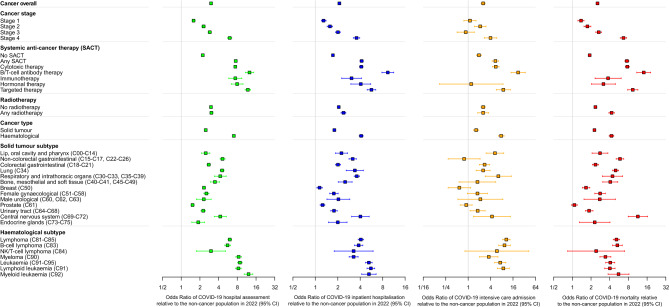
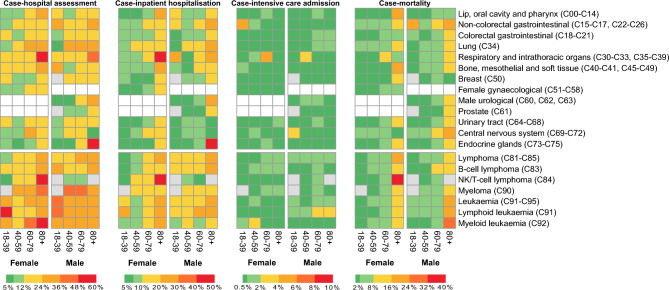
Patients with cancer are at increased risk of hospitalisation and mortality following severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. However, the SARS-CoV-2 phenotype evolution in patients with cancer since 2020 has not previously been described. We therefore evaluated SARS-CoV-2 on a UK populationscale from 01/11/2020-31/08/2022, assessing case-outcome rates of hospital assessment(s), intensive care admission and mortality. We observed that the SARS-CoV-2 disease phenotype has become less severe in patients with cancer and the non-cancer population. Case-hospitalisation rates for patients with cancer dropped from 30.58% in early 2021 to 7.45% in 2022 while case-mortality rates decreased from 20.53% to 3.25%. However, the risk of hospitalisation and mortality remains 2.10x and 2.54x higher in patients with cancer, respectively. Overall, the SARS-CoV-2 disease phenotype is less severe in 2022 compared to 2020 but patients with cancer remain at higher risk than the non-cancer population. Patients with cancer must therefore be empowered to live more normal lives, to see loved ones and families, while also being safeguarded with expanded measures to reduce the risk of transmission.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Becerril-Gaitan A, et al. Immunogenicity and risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection after coronavirus disease 2019 (COVID-19) vaccination in patients with cancer: A systematic review and meta-analysis. Eur. J. Cancer. 2022;160:243–260. doi: 10.1016/j.ejca.2021.10.014. - DOI - PMC - PubMed
-
- Gounant V, et al. Efficacy of severe acute respiratory syndrome coronavirus-2 vaccine in patients with thoracic Cancer: A prospective study supporting a third dose in patients with minimal serologic response after two vaccine doses. J. Thorac. Oncol. 2022;17:239–251. doi: 10.1016/j.jtho.2021.10.015. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
