

Surgical treatment of neonatal Cantrell pentalogy: a case report and literature review
- PMID: 37492795
- PMCID: PMC10364013
- DOI: 10.21037/acr-23-14
Surgical treatment of neonatal Cantrell pentalogy: a case report and literature review
Abstract
Background: Pentalogy of Cantrell (PC) is a congenital multiple malformation consisting of midline supraumbilical thoracoabdominal wall defects, anterior and pericardial diaphragm defects, lower sternum defects, ectopia cordis and various intracardiac anomalies, that present a distinctive challenge for care-providers and surgeons.
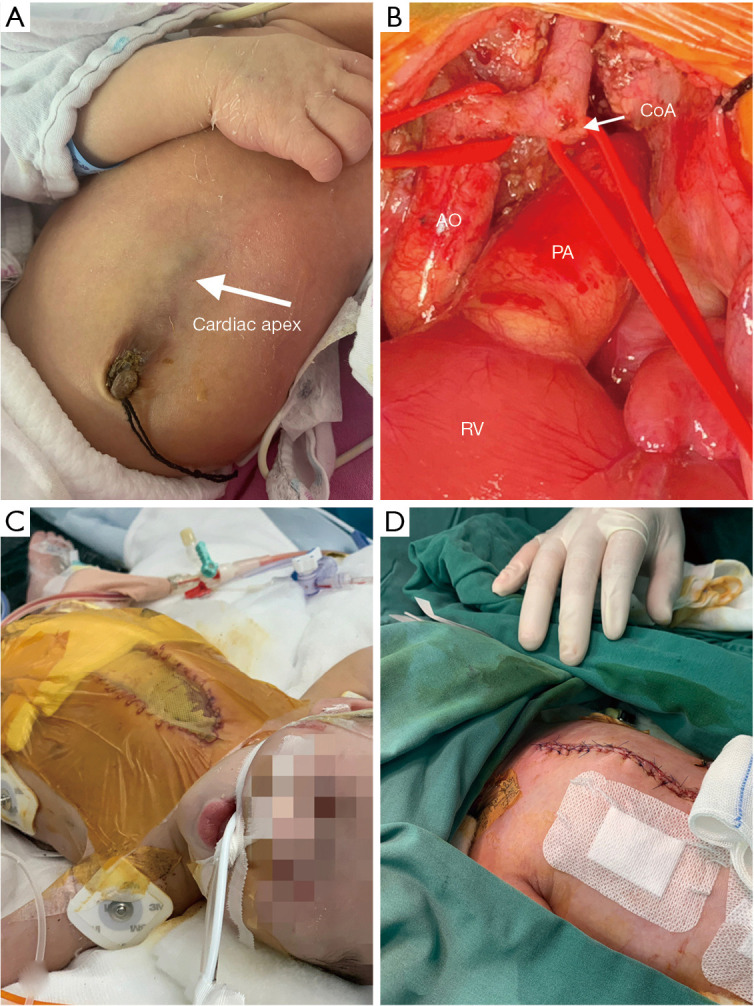
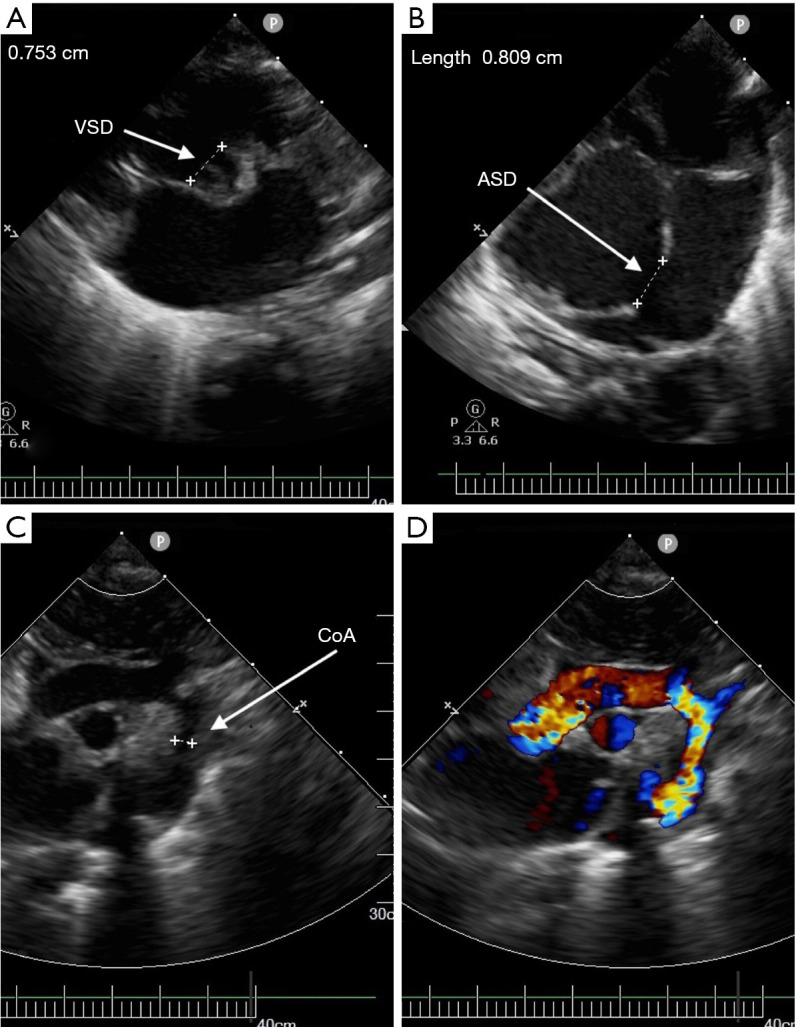
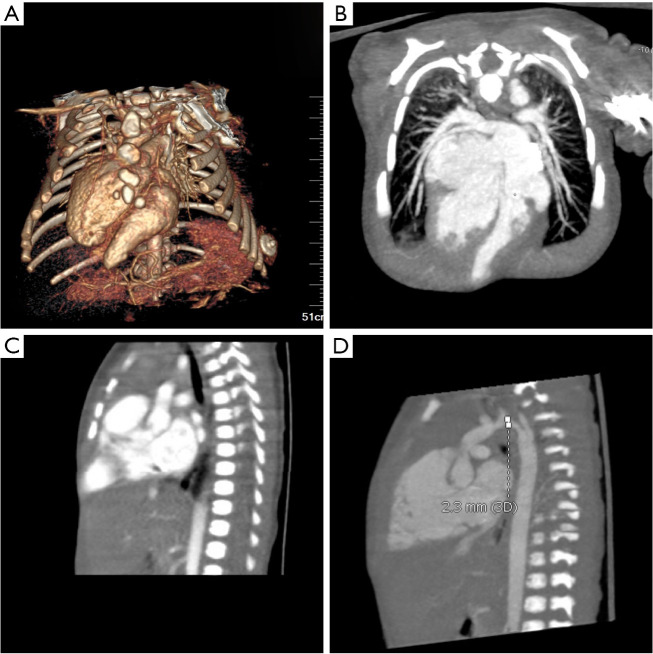
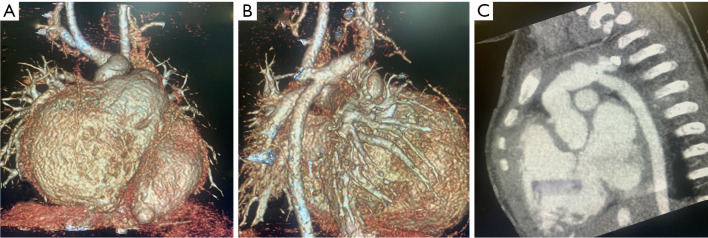
Case description: Cases of PC in twin pregnancies is rare. We report a new born infant, weighing 2,400 g, the younger twin. After birth, he was transferred to the Children's Hospital of Soochow University due to the prenatal echocardiography indicated that he has ventricular septal defect (VSD), atrial septal defect (ASD) and aortic arch hypoplasia. From the appearance, the lower end of sternum is suspiciously missing, the apical beating point is located at the lower edge of the median xiphoid process of sternum, and the upper abdominal muscle below the beating area is defective. He has the clinical and imaging features of complete type of PC. Three surgical operations were performed in the neonatal period, including end-to-side anastomosis of aortic arch under cardiopulmonary bypass (CPB), patch repair of VSD, repair of ASD, ligation of ductus arteriosus, correction of cardiac vascular malformation and repair of chest and abdominal wall defect, and the postoperative recoveries went smoothly.
Conclusions: PC is a rare congenital dysplasia, and its condition is complex. Our case shows that surgery is an effective treatment method, and the prognosis is related to the complexity of malformations.
Keywords: Cantrell; case report; neonate twin; pentalogy; surgical treatment.
2023 AME Case Reports. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://acr.amegroups.com/article/view/10.21037/acr-23-14/coif). The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Incomplete Pentalogy of Cantrell--A Case Report.Mymensingh Med J. 2016 Jan;25(1):153-7. Mymensingh Med J. 2016. PMID: 26931266
-
Pentalogy of Cantrell: a case report with pathologic findings.Pediatr Dev Pathol. 2004 Nov-Dec;7(6):649-52. doi: 10.1007/s10024-004-9104-5. Epub 2004 Dec 6. Pediatr Dev Pathol. 2004. PMID: 15630538
-
Twin pregnancy in which both fetuses have Cantrell's pentalogy: A case report and literature review.Eur J Obstet Gynecol Reprod Biol. 2021 May;260:64-69. doi: 10.1016/j.ejogrb.2021.03.016. Epub 2021 Mar 15. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 33743359 Review.
-
Ectopia Cordis Associated with Pentalogy of Cantrell-A Case Report.Rev Bras Ginecol Obstet. 2019 May;41(5):352-356. doi: 10.1055/s-0039-1679878. Epub 2019 Mar 25. Rev Bras Ginecol Obstet. 2019. PMID: 30912088 English.
-
Pentalogy of Cantrell: Case Report With Review of the Literature.Adv Neonatal Care. 2015 Aug;15(4):261-8. doi: 10.1097/ANC.0000000000000209. Adv Neonatal Care. 2015. PMID: 26225594 Review.
Cited by
-
The importance of designing a protector for a preterm and low birth weight infant with ectopia cordis.Clin Case Rep. 2024 Jan 3;12(1):e8403. doi: 10.1002/ccr3.8403. eCollection 2024 Jan. Clin Case Rep. 2024. PMID: 38173890 Free PMC article.
References
-
- Cantrell JR, Haller JA, Ravitch MM. A syndrome of congenital defects involving the abdominal wall, sternum, diaphragm, pericardium, and heart. Surg Gynecol Obstet 1958;107:602-14. - PubMed
-
- Toyama WM. Combined congenital defects of the anterior abdominal wall, sternum, diaphragm, pericardium, and heart: a case report and review of the syndrome. Pediatrics 1972;50:778-92. - PubMed
-
- Nayak S, Dash S P, Khatua M. Fetal anomaly: Pentalogy of Cantrell. IOSR J Dent Med Sci 2015;14:52-55.
Publication types
LinkOut - more resources
Full Text Sources