

Clinical benefit of range uncertainty reduction in proton treatment planning based on dual-energy CT for neuro-oncological patients
- PMID: 37493227
- PMCID: PMC10461272
- DOI: 10.1259/bjr.20230110
Clinical benefit of range uncertainty reduction in proton treatment planning based on dual-energy CT for neuro-oncological patients
Abstract
Objective: Several studies have shown that dual-energy CT (DECT) can lead to improved accuracy for proton range estimation. This study investigated the clinical benefit of reduced range uncertainty, enabled by DECT, in robust optimisation for neuro-oncological patients.
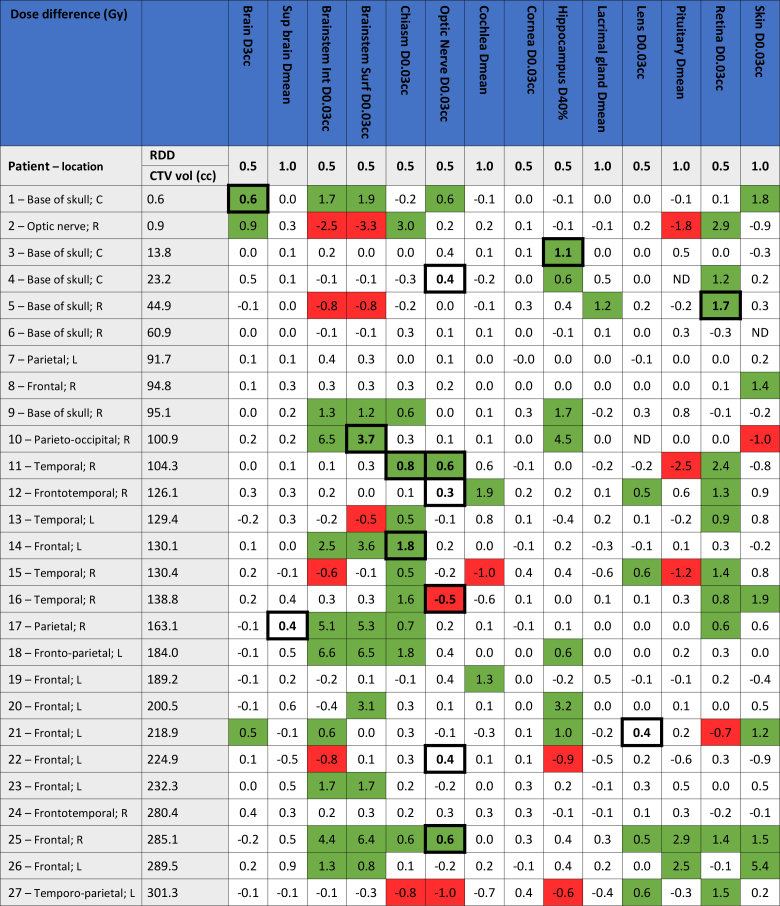
Methods: DECT scans for 27 neuro-oncological patients were included. Commercial software was applied to create stopping-power ratio (SPR) maps based on the DECT scan. Two plans were robustly optimised on the SPR map, keeping the beam and plan settings identical to the clinical plan. One plan was robustly optimised and evaluated with a range uncertainty of 3% (as used clinically; denoted 3%-plan); the second plan applied a range uncertainty of 2% (2%-plan). Both plans were clinical acceptable and optimal. The dose-volume histogram parameters were compared between the two plans. Two experienced neuro-radiation oncologists determined the relevant dose difference for each organ-at-risk (OAR). Moreover, the OAR toxicity levels were assessed.
Results: For 24 patients, a dose reduction >0.5/1 Gy (relevant dose difference depending on the OAR) was seen in one or more OARs for the 2%-plan; e.g. for brainstem D0.03cc in 10 patients, and hippocampus D40% in 6 patients. Furthermore, 12 patients had a reduction in toxicity level for one or two OARs, showing a clear benefit for the patient.
Conclusion: Robust optimisation with reduced range uncertainty allows for reduction of OAR toxicity, providing a rationale for clinical implementation. Based on these results, we have clinically introduced DECT-based proton treatment planning for neuro-oncological patients, accompanied with a reduced range uncertainty of 2%.
Advances in knowledge: This study shows the clinical benefit of range uncertainty reduction from 3% to 2% in robustly optimised proton plans. A dose reduction to one or more OARs was seen for 89% of the patients, and 44% of the patients had an expected toxicity level decrease.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
