

Evaluation of the Live-Attenuated Intranasal Respiratory Syncytial Virus (RSV) Vaccine RSV/6120/ΔNS2/1030s in RSV-Seronegative Young Children
- PMID: 37493269
- PMCID: PMC10873187
- DOI: 10.1093/infdis/jiad281
Evaluation of the Live-Attenuated Intranasal Respiratory Syncytial Virus (RSV) Vaccine RSV/6120/ΔNS2/1030s in RSV-Seronegative Young Children
Abstract
Background: Respiratory syncytial virus (RSV) is the leading cause of pediatric lower respiratory illness (LRI) and a vaccine for immunization of children is needed. RSV/6120/ΔNS2/1030s is a cDNA-derived live-vaccine candidate attenuated by deletion of the interferon antagonist NS2 gene and the genetically stabilized 1030s missense polymerase mutation in the polymerase, conferring temperature sensitivity.
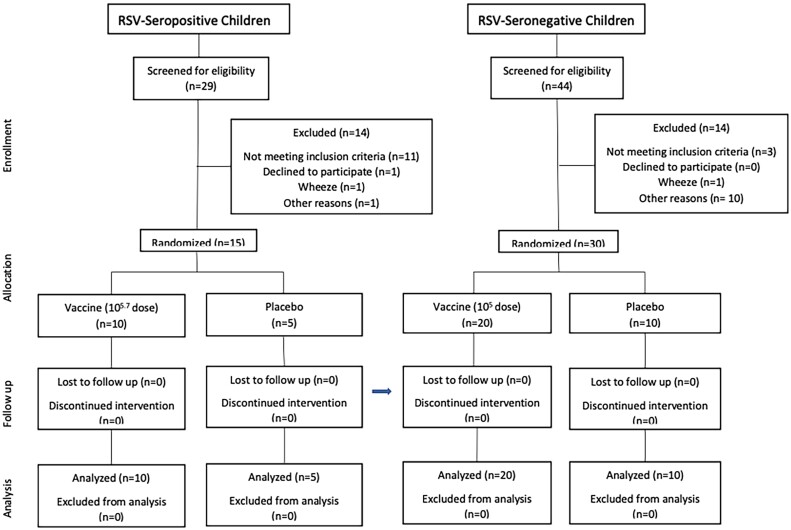
Methods: A single intranasal dose of RSV/6120/ΔNS2/1030s was evaluated in a double-blind, placebo-controlled trial (vaccine to placebo ratio, 2:1) at 105.7 plaque-forming units (PFU) in 15 RSV-seropositive 12- to 59-month-old children, and at 105 PFU in 30 RSV-seronegative 6- to 24-month-old children.
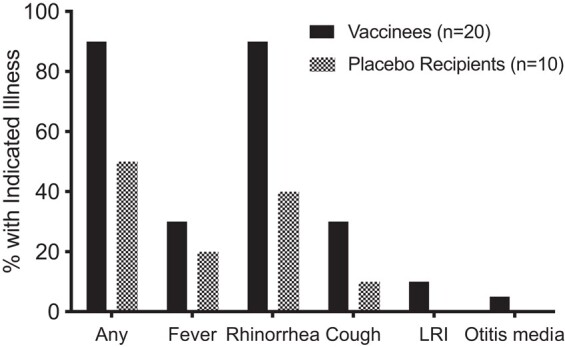
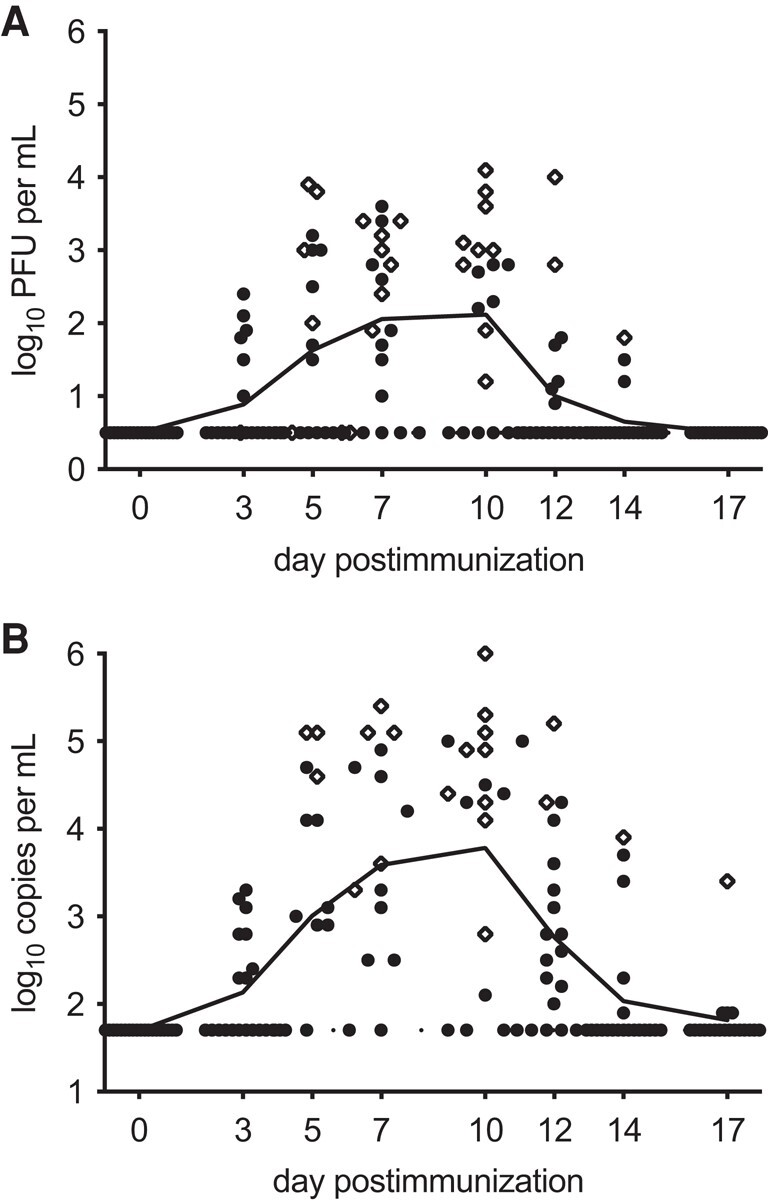
Results: RSV/6120/ΔNS2/1030s infected 100% of RSV-seronegative vaccinees and was immunogenic (geometric mean RSV plaque-reduction neutralizing antibody titer [RSV-PRNT], 1:91) and genetically stable. Mild rhinorrhea was detected more frequently in vaccinees (18/20 vaccinees vs 4/10 placebo recipients, P = .007), and LRI occurred in 1 vaccinee during a period when only vaccine virus was detected. Following the RSV season, 5 of 16 vaccinees had ≥4-fold rises in RSV-PRNT with significantly higher titers than 4 of 10 placebo recipients with rises (1:1992 vs 1:274, P = .02). Thus, RSV/6120/ΔNS2/1030s primed for substantial anamnestic neutralizing antibody responses following naturally acquired RSV infection.
Conclusions: RSV/6120/ΔNS2/1030s is immunogenic and genetically stable in RSV-seronegative children, but the frequency of rhinorrhea in vaccinees exceeded that in placebo recipients.
Clinical trials registration: NCT03387137.
Keywords: RSV; intranasal vaccine; live-attenuated; pediatric; vaccine.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest . C. L., P. L. C., and U. J. B. are inventors on US patents pertaining to this vaccine candidate and its attenuating mutations. R. A. K. receives additional grant funding from Sanofi through her institution. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Karron RA. Preventing respiratory syncytial virus (RSV) disease in children. Science 2021; 372:686–7. - PubMed
-
- Wang X, Li Y, Mei X, Bushe E, Campbell H, Nair H. Global hospital admissions and in-hospital mortality associated with all-cause and virus-specific acute lower respiratory infections in children and adolescents aged 5–19 years between 1995 and 2019: a systematic review and modelling study. BMJ Glob Health 2021; 6:e006014. - PMC - PubMed
-
- Karron RA, Black RE. Determining the burden of respiratory syncytial virus disease: the known and the unknown. Lancet 2017; 390:917–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
