

The Role of Alternative Lymph Node Classification Systems in Gastroenteropancreatic Neuroendocrine Neoplasms (GEP-NEN): Superiority of a LODDS Scheme Over N Category in Pancreatic NEN (pNEN)
- PMID: 37494059
- PMCID: PMC10370471
- DOI: 10.1055/a-2102-7694
The Role of Alternative Lymph Node Classification Systems in Gastroenteropancreatic Neuroendocrine Neoplasms (GEP-NEN): Superiority of a LODDS Scheme Over N Category in Pancreatic NEN (pNEN)
Abstract
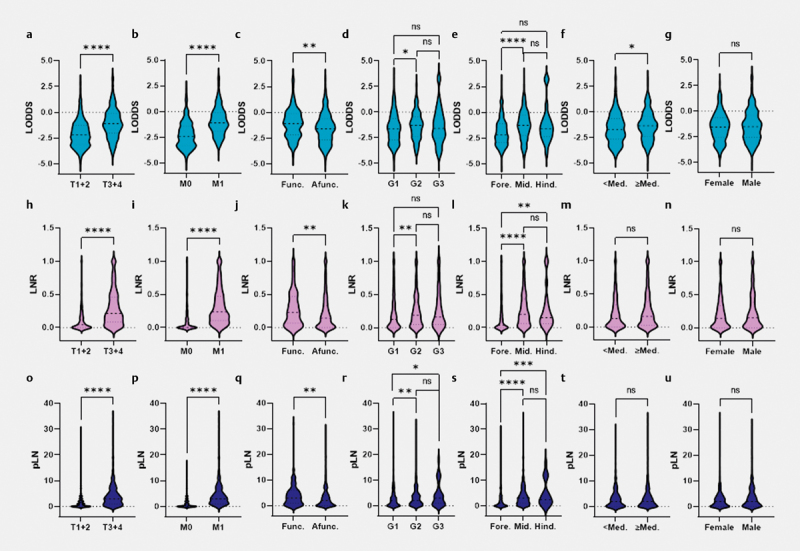
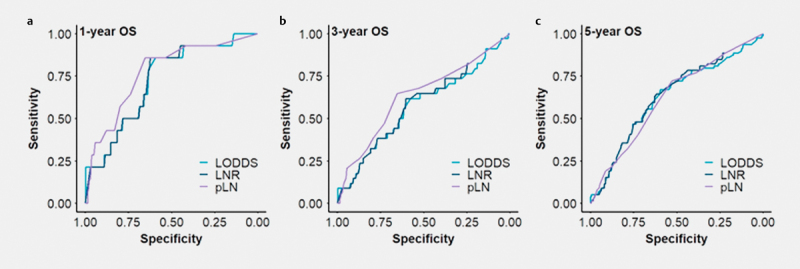
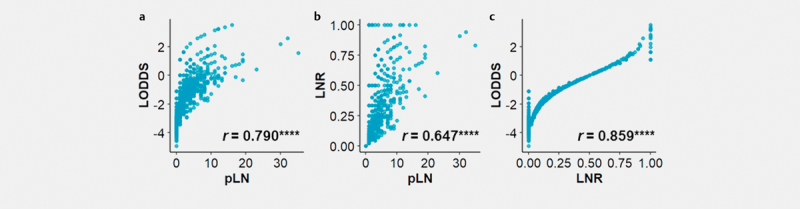
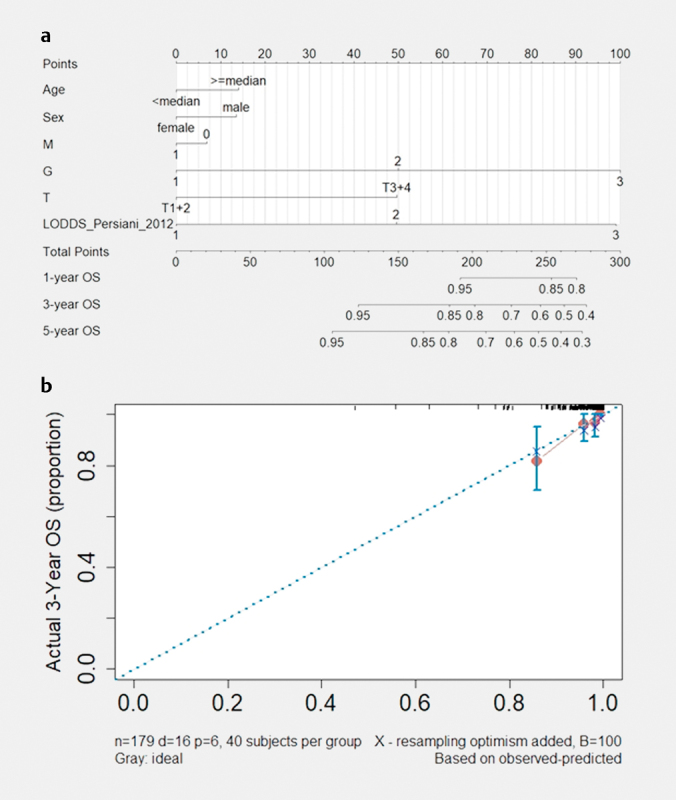
Lymph node (LN) involvement in gastroenteropancreatic neuroendocrine neoplasms (GEP-NEN) has been reported to have prognostic and therapeutic implications. Numerous novel LN classifications exist; however, no comparison of their prognostic performance for GEP-NEN has been done yet. Using a nationwide cohort from the German Neuroendocrine Tumor (NET) Registry, the prognostic and discriminatory power of different LN ratio (LNR) and log odds of metastatic LN (LODDS) classifications were investigated using multivariate Cox regression and C-statistics in 671 patients with resected GEP-NEN. An increase in positive LN (pLN), LNR, and LODDS was associated with advanced tumor stages, distant metastases, and hormonal functionality. However, none of the alternative LN classifications studied showed discriminatory superiority in predicting prognosis over the currently used N category. Interestingly, in a subgroup analysis, one LODDS classification was identified that might be most appropriate for patients with pancreatic NEN (pNEN). On this basis, a nomogram was constructed to estimate the prognosis of pNEN patients after surgery. In conclusion, a more accurate classification of LN status may allow a more precise prediction of overall survival and provide the basis for individualized strategies for postoperative treatment and surveillance especially for patients with pNEN.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Modlin I M, Oberg K, Chung D C. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008;9:61–72. - PubMed
-
- Modlin I M, Lye K D, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer. 2003;97:934–959. - PubMed
-
- Detjen K, Hammerich L, Özdirik B. Models of gastroenteropancreatic neuroendocrine neoplasms: current status and future directions. Neuroendocrinology. 2021;111:217–236. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical