

Impact of cytogenetic abnormalities on the risk of disease progression in solitary bone plasmacytomas
- PMID: 37494698
- PMCID: PMC10731916
- DOI: 10.1182/blood.2023021187
Impact of cytogenetic abnormalities on the risk of disease progression in solitary bone plasmacytomas
Abstract
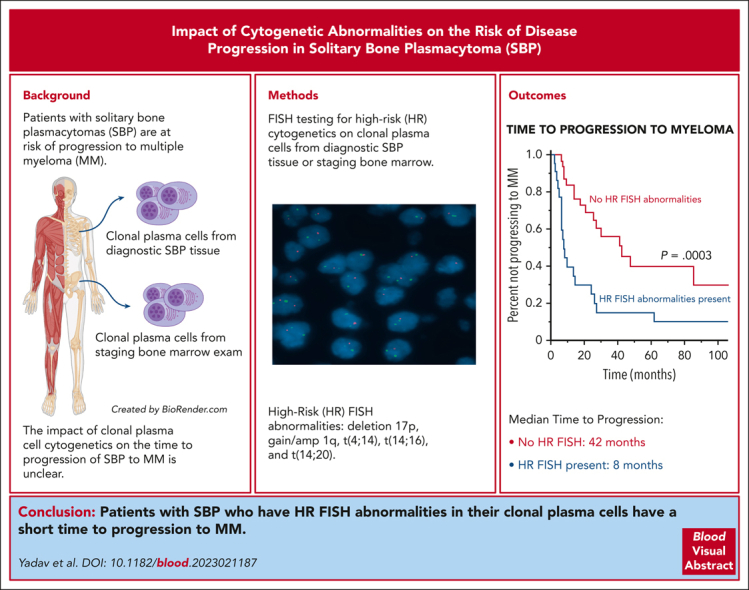
Most patients with solitary bone plasmacytomas (SBP) progress to multiple myeloma (MM) after definitive radiation therapy as their primary treatment. Whether the presence of high-risk (HR) cytogenetic abnormalities by fluorescence in situ hybridization (FISH) in the clonal plasma cells, obtained either directly from the diagnostic SBP tissue or the corresponding bone marrow examination at the time of diagnosis, is associated with a shorter time to progression (TTP) to MM is unknown. This study evaluated all patients diagnosed with SBP at the Mayo Clinic from January 2012 to July 2022. The presence of del(17p), t(14;16), t(4;14), or +1q (gain or amplification) by FISH in clonal plasma cells was defined as HR. A total of 114 patients were included in this cohort, and baseline FISH was available for 55 patients (48%), of which 22 were classified as HR (40%). The median TTP to MM for patients with SBP and HR FISH was 8 months (95% confidence interval [CI], 6.3-26) compared with 42 months (95% CI, 25-not reached [NR]) in patients with SBP without HR FISH (P < .001). In a multivariate analysis, only HR FISH was a significant predictor for shorter TTP to MM, independent of minimal marrow involvement and an abnormal serum free light chain ratio at diagnosis. Deletion (17p) and gain 1q abnormalities were the most common FISH abnormalities responsible for the short TTP to MM. Thus, assessing for HR FISH abnormalities in clonal plasma cells derived from either the diagnostic SBP tissue or the staging bone marrow examination of patients with newly diagnosed SBP is feasible and prognostic for a shorter TTP to MM.
© 2023 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: R.F. reports consulting for AbbVie, Adaptive Biotechnologies, AMGEN, AstraZeneca, Bayer, Binding Site, Bristol Myers Squibb (Celgene), Millenium Takeda, Janssen, Juno, Kite, Merck, Pfizer, Pharmacyclics, Regeneron, and Sanofi; is a member of scientific advisory boards for Adaptive Biotechnologies, Caris Life Sciences, and ONCOtracker; is a member of board of directors for Antengene (for profit) and AZBio (not for profit); and has a patent for fluorescence in situ hybridization in multiple myeloma receiving ∼$2000 per year. The remaining authors declare no competing financial interests.
Figures


Comment in
-
When a solitary plasmacytoma is just the beginning….Blood. 2023 Nov 30;142(22):1849-1850. doi: 10.1182/blood.2023021859. Blood. 2023. PMID: 38032673 No abstract available.
References
-
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–e548. - PubMed
-
- Tsang RW, Campbell BA, Goda JS, et al. radiation therapy for solitary plasmacytoma and multiple myeloma: guidelines from the International Lymphoma Radiation Oncology Group. Int J Radiat Oncol Biol Phys. 2018;101(4):794–808. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
