

The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease
- PMID: 37495237
- PMCID: PMC10529191
- DOI: 10.1136/ard-2023-224575
The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease
Abstract
Objective: Calcium pyrophosphate deposition (CPPD) disease is prevalent and has diverse presentations, but there are no validated classification criteria for this symptomatic arthritis. The American College of Rheumatology (ACR) and EULAR have developed the first-ever validated classification criteria for symptomatic CPPD disease.
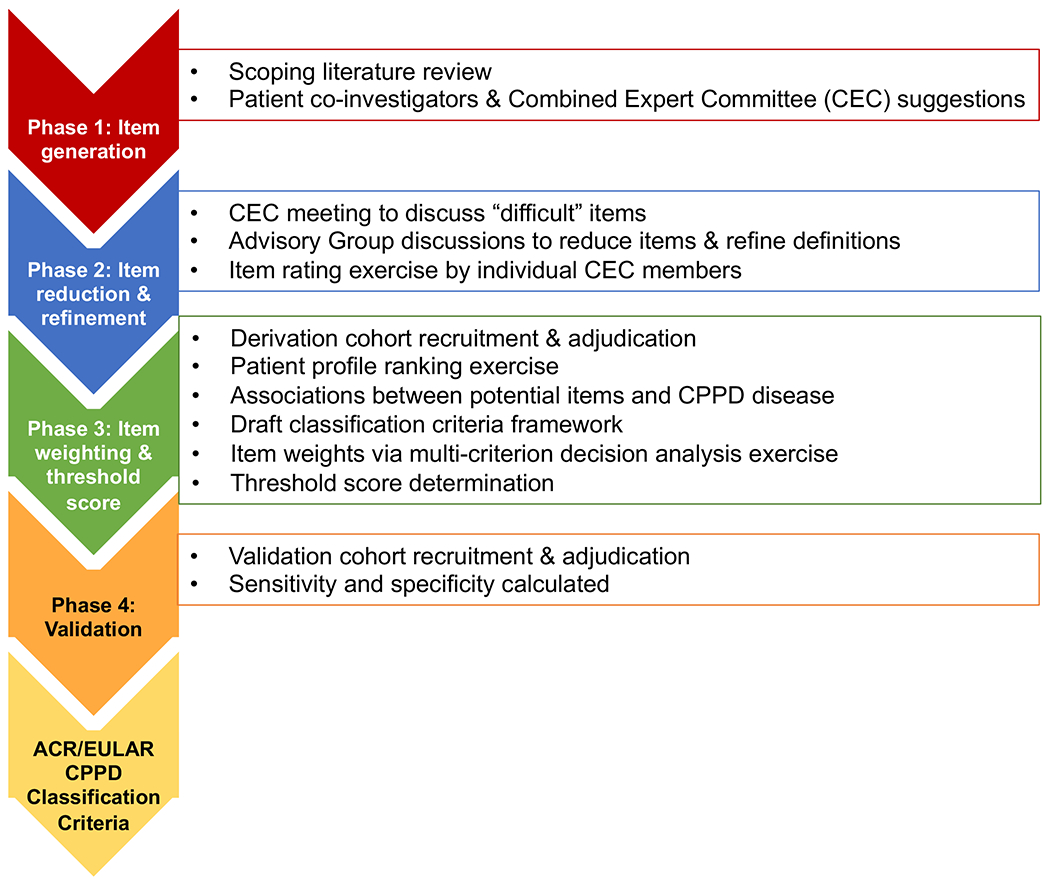
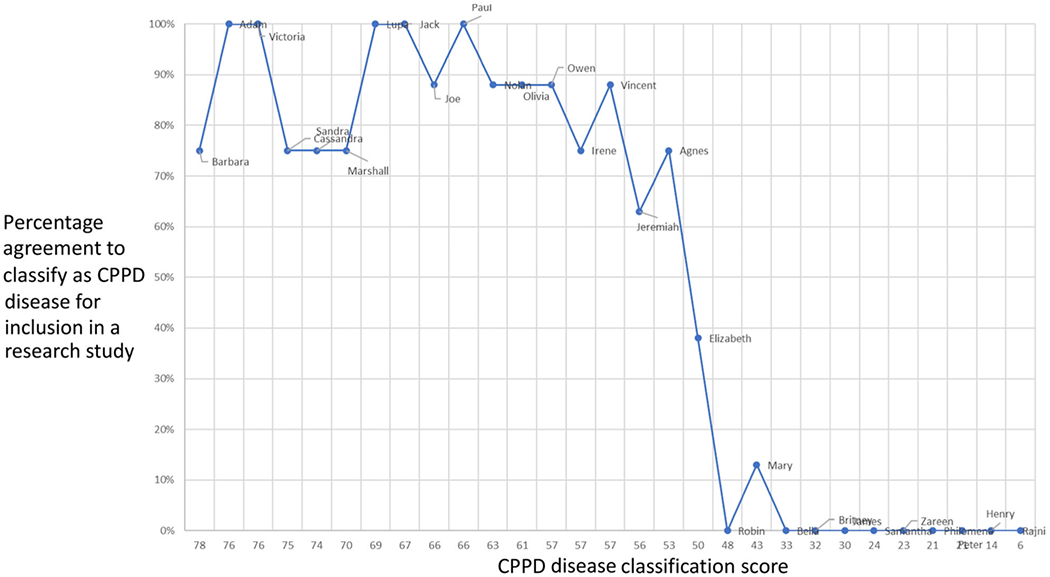
Methods: Supported by the ACR and EULAR, a multinational group of investigators followed established methodology to develop these disease classification criteria. The group generated lists of candidate items and refined their definitions, collected de-identified patient profiles, evaluated strengths of associations between candidate items and CPPD disease, developed a classification criteria framework, and used multi-criterion decision analysis to define criteria weights and a classification threshold score. The criteria were validated in an independent cohort.
Results: Among patients with joint pain, swelling, or tenderness (entry criterion) whose symptoms are not fully explained by an alternative disease (exclusion criterion), the presence of crowned dens syndrome or calcium pyrophosphate crystals in synovial fluid are sufficient to classify a patient as having CPPD disease. In the absence of these findings, a score>56 points using weighted criteria, comprising clinical features, associated metabolic disorders, and results of laboratory and imaging investigations, can be used to classify as CPPD disease. These criteria had a sensitivity of 92.2% and specificity of 87.9% in the derivation cohort (190 CPPD cases, 148 mimickers), whereas sensitivity was 99.2% and specificity was 92.5% in the validation cohort (251 CPPD cases, 162 mimickers).
Conclusion: The 2023 ACR/EULAR CPPD disease classification criteria have excellent performance characteristics and will facilitate research in this field.
Keywords: Autoimmune Diseases; Immune Complex Diseases; Immune System Diseases.
© Author(s) (or their employer(s)) 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
-
- Zhang W, Doherty M, Bardin T, Barskova V, Guerne PA, Jansen TL, et al. European League Against Rheumatism recommendations for calcium pyrophosphate deposition. Part I: terminology and diagnosis. Ann Rheum Dis. 2011;70(4):563–70. - PubMed
-
- Salaffi F, De Angelis R, Grassi W. Prevalence of musculoskeletal conditions in an Italian population sample: results of a regional community-based study. I. The MAPPING study. Clinical and experimental rheumatology. 2005;23(6):819–28. - PubMed
-
- Ramonda R, Musacchio E, Perissinotto E, Sartori L, Punzi L, Corti M, et al. Prevalence of chondrocalcinosis in Italian subjects from northeastern Italy. The Pro. VA (PROgetto Veneto Anziani) study. Clin Exp Rheumatol. 2009;27(6):981–4. - PubMed
-
- Felson D, Anderson J, Naimark A, Kannel W, Meenan R. The prevalence of chondrocalcinosis in the elderly and its association with knee osteoarthritis: the Framingham Study. The Journal of rheumatology. 1989;16(9):1241–5. - PubMed