

Efficacy and safety comparison between axillary lymph node dissection with no axillary surgery in patients with sentinel node-positive breast cancer: a systematic review and meta-analysis
- PMID: 37495945
- PMCID: PMC10369839
- DOI: 10.1186/s12893-023-02101-8
Efficacy and safety comparison between axillary lymph node dissection with no axillary surgery in patients with sentinel node-positive breast cancer: a systematic review and meta-analysis
Abstract
Background: This systematic review and meta-analysis aimed to study the evidence on the efficacy and safety of omitting axillary lymph node dissection (ALND) for patients with clinically node-negative but sentinel lymph node (SLN)-positive breast cancer using all the available evidence.
Methods: The Embase, Medline, and Cochrane Library databases were searched through February 25, 2023. Original trials that compared only the sentinel lymph node biopsy (SLNB) with ALND as the control group for patients with clinically node-negative but SLN-positive breast cancer were included. The primary outcomes were axillary recurrence rate, total recurrence rate, disease-free survival (DFS), and overall survival (OS). Meta-analyses were performed to compare the odds ratio (OR) in rates and the hazard ratios (HR) in time-to-event outcomes between both interventions. Based on different study designs, tools in the revised Cochrane risk of bias tool were used for randomized trials and the risk of bias in nonrandomized studies of interventions to assess the risk of bias for each included article. Funnel plots and Egger's test were used for the publication's bias assessment.
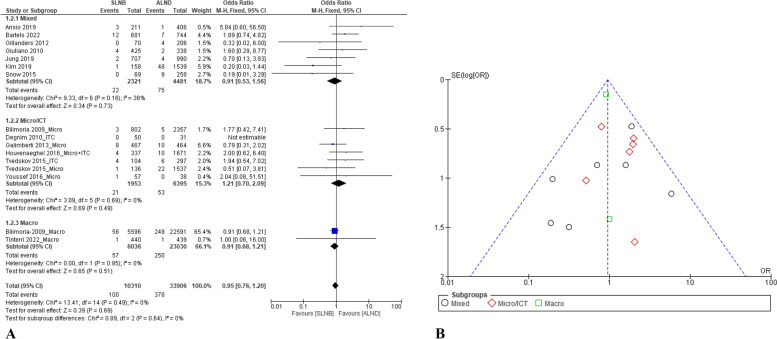
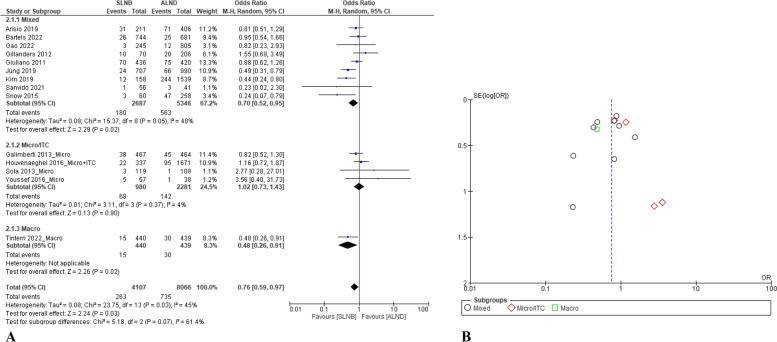
Results: In total, 30 reports from 26 studies were included in the systematic review (9 reports of RCTs, 21 reports of retrospective cohort studies). According to our analysis, omitting ALND in patients with clinically node-negative but SLN-positive breast cancer had a similar axillary recurrence rate (OR = 0.95, 95% confidence interval (CI): 0.76-1.20), DFS (HR = 1.02, 95% CI: 0.89-1.16), and OS (HR = 0.97, 95% CI: 0.92-1.03), but caused a significantly lower incidence of adverse events and benefited in locoregional recurrence rate (OR = 0.76, 95% CI: 0.59-0.97) compared with ALND.
Conclusion: For patients with clinically node-negative but SLN-positive breast cancer (no matter the number of the positive SLN), this review showed that SLNB alone had a similar axillary recurrence rate, DFS, and OS, but caused a significantly lower incidence of adverse events and showed a benefit for the locoregional recurrence compared with ALND. An OS benefit was found in the Macro subset that used SLNB alone versus complete ALND. Therefore, omitting ALND is feasible in this setting.
Trial registration: CRD 42023397963.
Keywords: Axillary lymph node dissection; Breast cancer; Sentinel lymph node biopsy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Axillary lymph node dissection vs. sentinel node biopsy for early-stage clinically node-negative breast cancer: a systematic review and meta-analysis.Arch Gynecol Obstet. 2022 Oct;306(4):1221-1234. doi: 10.1007/s00404-022-06458-8. Epub 2022 Mar 5. Arch Gynecol Obstet. 2022. PMID: 35249123
-
Recommendation for axillary lymph node dissection in women with early breast cancer and sentinel node metastasis: A systematic review and meta-analysis of randomized controlled trials using the GRADE system.Int J Surg. 2016 Oct;34:73-80. doi: 10.1016/j.ijsu.2016.08.022. Epub 2016 Aug 22. Int J Surg. 2016. PMID: 27562691
-
Comparing Early-Stage Breast Cancer Patients with Sentinel Lymph Node Metastasis with and without Completion Axillary Lymph Node Dissection: A Systematic Review and Meta-Analysis.Asian Pac J Cancer Prev. 2022 Aug 1;23(8):2561-2571. doi: 10.31557/APJCP.2022.23.8.2561. Asian Pac J Cancer Prev. 2022. PMID: 36037108 Free PMC article.
-
Oncological Safety of Skipping Axillary Lymph Node Dissection in Patients with Clinical N0, Sentinel Node-Positive Breast Cancer Undergoing Total Mastectomy.Ann Surg Oncol. 2024 May;31(5):3168-3176. doi: 10.1245/s10434-024-15049-7. Epub 2024 Feb 17. Ann Surg Oncol. 2024. PMID: 38368292 Free PMC article.
-
Long-term survival after sentinel lymph node biopsy or axillary lymph node dissection in pN0 breast cancer patients: a population-based study.Breast Cancer Res Treat. 2022 Dec;196(3):613-622. doi: 10.1007/s10549-022-06746-6. Epub 2022 Oct 7. Breast Cancer Res Treat. 2022. PMID: 36207619
Cited by
-
Predictive value of MRI-based deep learning model for lymphovascular invasion status in node-negative invasive breast cancer.Sci Rep. 2024 Jul 13;14(1):16204. doi: 10.1038/s41598-024-67217-0. Sci Rep. 2024. PMID: 39003325 Free PMC article.
-
Prediction of the number of positive axillary lymph nodes according to sentinel lymph node involvement and biological subtypes in patients receiving neoadjuvant chemotherapy.BMC Surg. 2024 Jul 19;24(1):213. doi: 10.1186/s12893-024-02500-5. BMC Surg. 2024. PMID: 39030524 Free PMC article.
-
The prognostic analysis of further axillary dissection in breast cancer with 1-2 positive sentinel lymph nodes undergoing mastectomy.Front Oncol. 2024 Aug 5;14:1406981. doi: 10.3389/fonc.2024.1406981. eCollection 2024. Front Oncol. 2024. PMID: 39161383 Free PMC article.
References
-
- Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Ashikaga T, Weaver DL, Miller BJ, Jalovec LM, Frazier TG, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase III trial. Lancet Oncol. 2007;8(10):881–888. doi: 10.1016/S1470-2045(07)70278-4. - DOI - PubMed
-
- Manca G, Rubello D, Tardelli E, Giammarile F, Mazzarri S, Boni G, Chondrogiannis S, Marzola MC, Chiacchio S, Ghilli M, et al. Sentinel lymph node biopsy in breast cancer: indications, contraindications, and controversies. Clin Nucl Med. 2016;41(2):126–133. doi: 10.1097/RLU.0000000000000985. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
