

Enabling endpoint development for interventional clinical trials in individuals with Angelman syndrome: a prospective, longitudinal, observational clinical study (FREESIAS)
- PMID: 37495977
- PMCID: PMC10373389
- DOI: 10.1186/s11689-023-09494-w
Enabling endpoint development for interventional clinical trials in individuals with Angelman syndrome: a prospective, longitudinal, observational clinical study (FREESIAS)
Abstract
Background: Angelman syndrome (AS) is a rare neurodevelopmental disorder characterized by the absence of a functional UBE3A gene, which causes developmental, behavioral, and medical challenges. While currently untreatable, comprehensive data could help identify appropriate endpoints assessing meaningful improvements in clinical trials. Herein are reported the results from the FREESIAS study assessing the feasibility and utility of in-clinic and at-home measures of key AS symptoms.
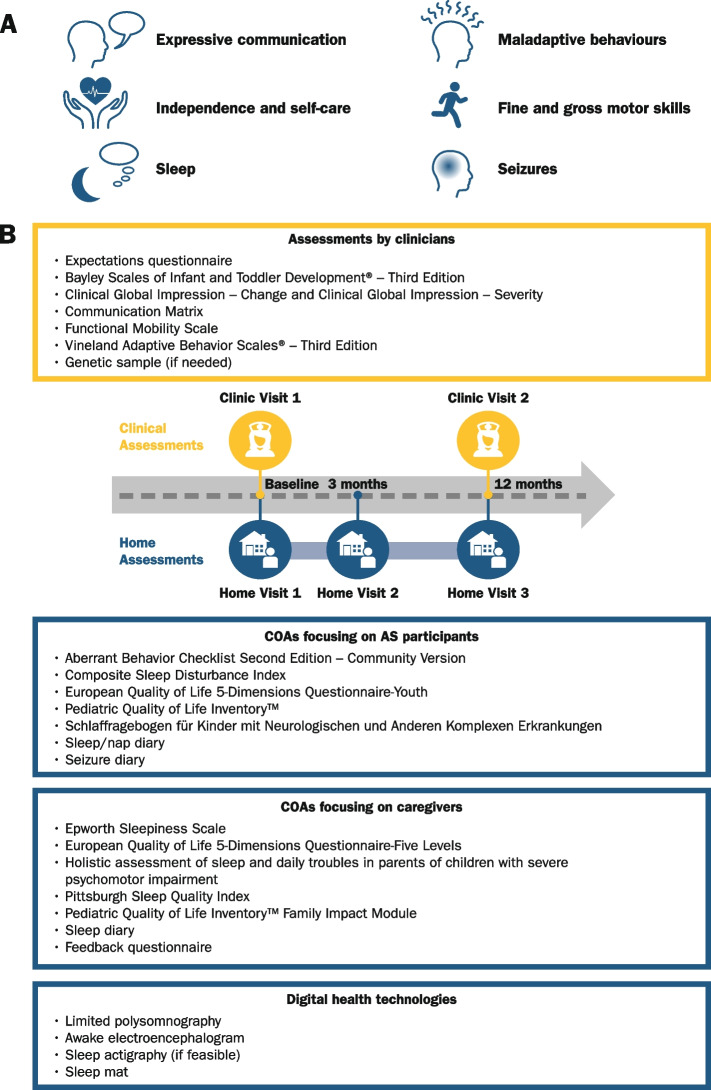
Methods: Fifty-five individuals with AS (aged < 5 years: n = 16, 5-12 years: n = 27, ≥ 18 years: n = 12; deletion genotype: n = 40, nondeletion genotype: n = 15) and 20 typically developing children (aged 1-12 years) were enrolled across six USA sites. Several clinical outcome assessments and digital health technologies were tested, together with overnight 19-lead electroencephalography (EEG) and additional polysomnography (PSG) sensors. Participants were assessed at baseline (Clinic Visit 1), 12 months later (Clinic Visit 2), and during intermittent home visits.
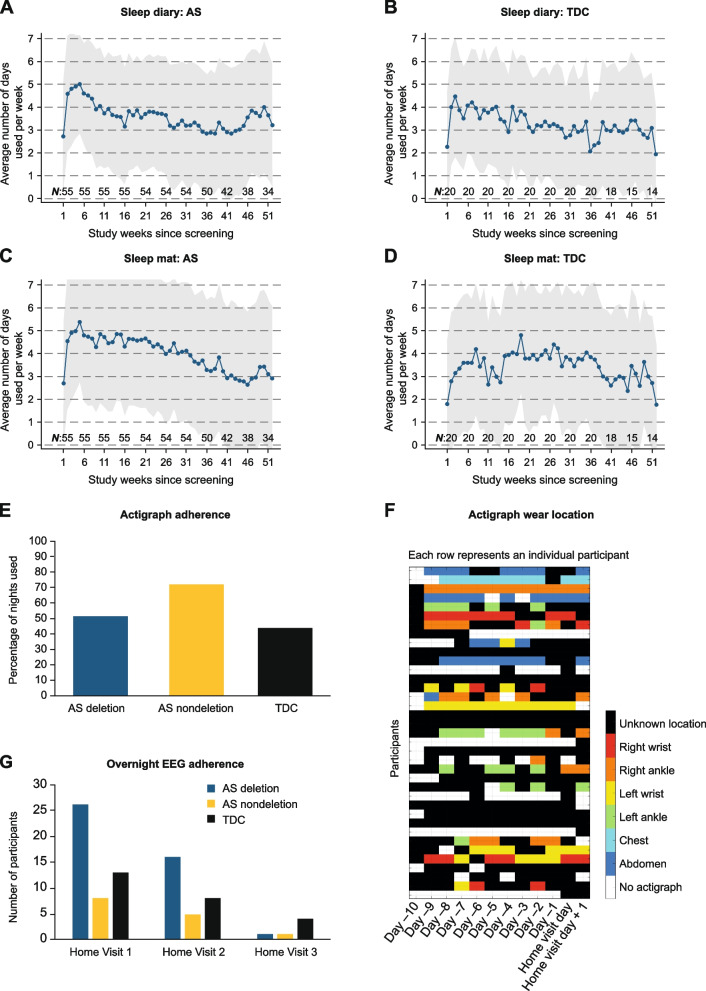
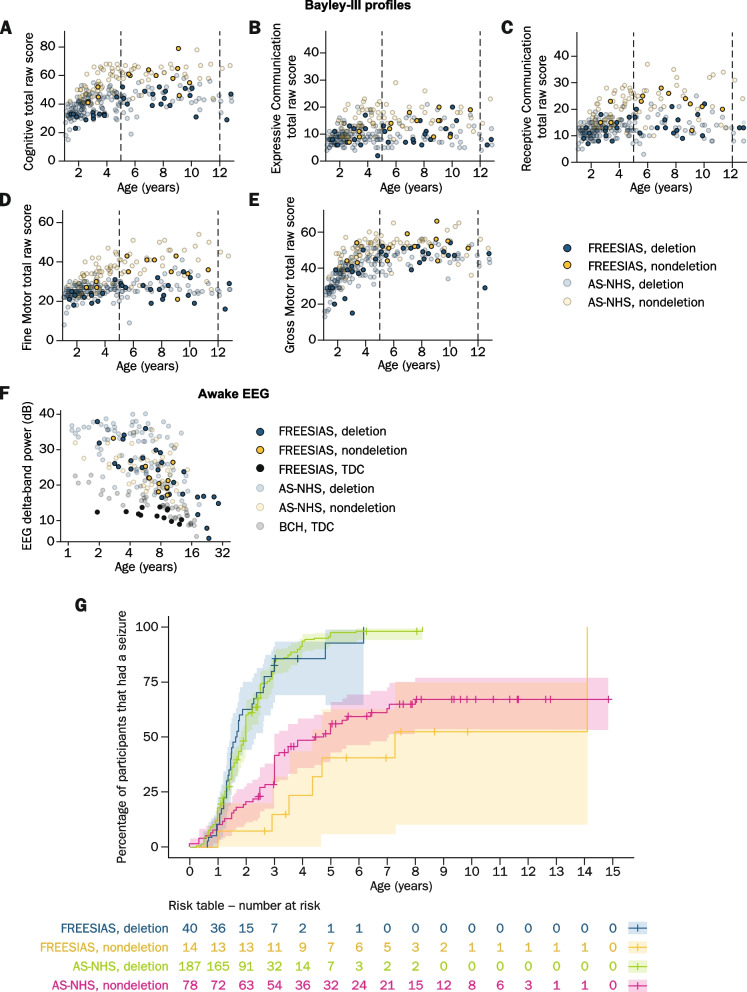
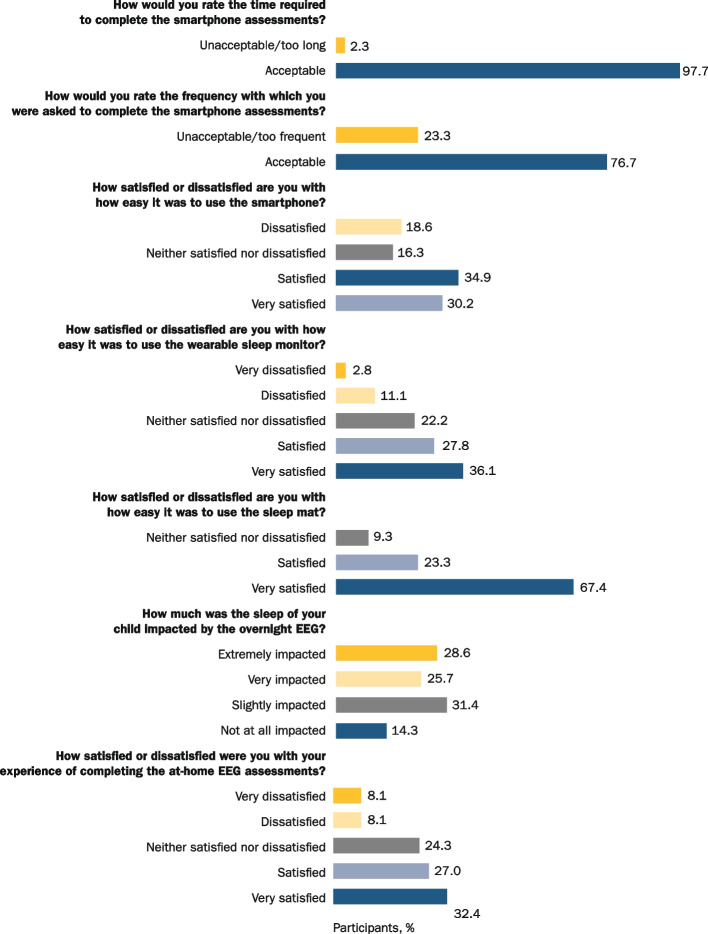
Results: The participants achieved high completion rates for the clinical outcome assessments (adherence: 89-100% [Clinic Visit 1]; 76-91% [Clinic Visit 2]) and varied feasibility of and adherence to digital health technologies. The coronavirus disease 2019 (COVID-19) pandemic impacted participants' uptake of and/or adherence to some measures. It also potentially impacted the at-home PSG/EEG recordings, which were otherwise feasible. Participants achieved Bayley-III results comparable to the available natural history data, showing similar scores between individuals aged ≥ 18 and 5-12 years. Also, participants without a deletion generally scored higher on most clinical outcome assessments than participants with a deletion. Furthermore, the observed AS EEG phenotype of excess delta-band power was consistent with prior reports.
Conclusions: Although feasible clinical outcome assessments and digital health technologies are reported herein, further improved assessments of meaningful AS change are needed. Despite the COVID-19 pandemic, remote assessments facilitated high adherence levels and the results suggested that at-home PSG/EEG might be a feasible alternative to the in-clinic EEG assessments. Taken altogether, the combination of in-clinic/at-home clinical outcome assessments, digital health technologies, and PSG/EEG may improve protocol adherence, reduce patient burden, and optimize study outcomes in AS and other rare disease populations.
Keywords: Angelman syndrome; Clinical outcome assessments; Clinical trials; Digital health technology; EEG; Endpoint development; Natural history; Sleep; UBE3A.
© 2023. The Author(s).
Conflict of interest statement
JT is an employee of F. Hoffmann-La Roche Ltd.
CAB is the Principal Investigator for clinical trials in Angelman syndrome sponsored by F. Hoffmann-La Roche Ltd. and Ionis Pharmaceuticals Inc. He is also the Principal Investigator for research trials in achondroplasia sponsored by BioMarin, Pfizer Pharmaceuticals, and Ascendis Pharmaceuticals. He is a co-investigator in the Undiagnosed Research Network grant sponsored by the NIH. He is a consultant for Best Doctors Inc.
TJB has been a paid consultant for F. Hoffmann-La Roche Ltd.
LMB has been a paid consultant for F. Hoffmann-La Roche Ltd. and Ionis Pharmaceuticals Inc. regarding clinical trial design and is/has been a principal investigator on trials sponsored by F. Hoffmann-La Roche Ltd., Ionis Pharmaceuticals Inc., Biogen, and Ovid Therapeutics.
MB is an employee of F. Hoffmann-La Roche Ltd.
RC is an employee of Ionis Pharmaceuticals Inc. SJ serves as a consultant for Roche Pharmaceuticals.
RWK was an employee of Biogen and is an employee of Ionis Pharmaceuticals Inc.
MLK was an employee of F. Hoffmann-La Roche Ltd.
COL was a principal investigator or co-investigator for clinical trials in Angelman syndrome sponsored by Ovid, F. Hoffmann-La Roche Ltd., GeneTx, Biogen, and Ionis Pharmaceuticals Inc. All funds from clinical trials were paid to Rush University Medical Center and COL did not keep any personal funds.
MTM was an employee of F. Hoffmann-La Roche Ltd.
DN is an employee of F. Hoffmann-La Roche Ltd.
KP was an employee of Biogen.
AR has been a paid consultant and has received research support from F. Hoffmann-La Roche Ltd. He has also received recent research support from BioMarin, CRE Medical, Encoded, LouLou Foundation, Neuroelectrics, SSADH Foundation, and Takeda. He is co-founder and has equity in PrevEp Inc. and Galibra Inc.
ACW has been a paid consultant for F. Hoffmann-La Roche Ltd.
AS has been a paid consultant for F. Hoffmann-La Roche Ltd.
MDS was Principal Investigator or co-investigator for clinical trials in Angelman syndrome sponsored by F. Hoffmann-La Roche Ltd., Biogen, and Ionis Pharmaceuticals Inc.; and served as a consultant for Ionis Pharmaceuticals Inc. during the design of the trial before study startup. All funds were paid to the University of North Carolina, and MDS did not receive any personal funds.
LS is an employee of F. Hoffmann-La Roche Ltd.
WHT was a paid consultant for F. Hoffmann-La Roche Ltd.
BV is an employee of F. Hoffmann-La Roche Ltd.
AW was a paid consultant for F. Hoffmann-La Roche Ltd. And Ovid.
JFH is an employee of F. Hoffmann-La Roche Ltd.
EBK has received funding from Acadia, Alcobra, AMO, Asuragen, Avexis, Biogen, BioMarin, Cydan, Erydel Fulcrum, GeneTx, GW, Ionis Pharmaceuticals Inc., Jaguar, Lumos, Marinus, Neuren, Neurogene, Neurotrope, Novartis, Orphazyme, Ovid, Retrophin, Roche, Seaside Therapeutics, Taysha, Tetra, Ultragenyx, Yamo, Zynerba, and Vtesse/Sucampo/Mallinckrodt Pharmaceuticals, to consult on trial design or run clinical or lab validation trials in genetic neurodevelopmental or neurodegenerative disorders, all of which is directed to RUMC in support of rare disease programs; EBK receives no personal funds and RUMC has no relevant financial interest in any of the commercial entities listed.
Figures
References
-
- Mertz LGB, Christensen R, Vogel I, Hertz JM, Brøndum Nielsen K, Grønskov K, et al. Angelman syndrome in Denmark. Birth incidence, genetic findings, and age at diagnosis. Am J Med Genet A. 2013;161:2197–203; 10.1002/ajmg.a.36058. - PubMed
