

Comparative cardiovascular outcomes in type 2 diabetes patients taking dapagliflozin versus empagliflozin: a nationwide population-based cohort study
- PMID: 37496050
- PMCID: PMC10373410
- DOI: 10.1186/s12933-023-01911-7
Comparative cardiovascular outcomes in type 2 diabetes patients taking dapagliflozin versus empagliflozin: a nationwide population-based cohort study
Abstract
Background: Sodium-glucose co-transporter-2 inhibitors displayed cardiovascular benefits in type 2 diabetes mellitus in previous studies; however, there were some heterogeneities regarding respective cardiovascular outcomes within the class. Furthermore, their efficacies in Asians, females, and those with low cardiovascular risks were under-represented. Thus, we compared the cardiovascular outcomes between new users of dapagliflozin and empagliflozin in a broad range of patients with type 2 diabetes mellitus using a nationwide population-based real-world cohort from Korea.
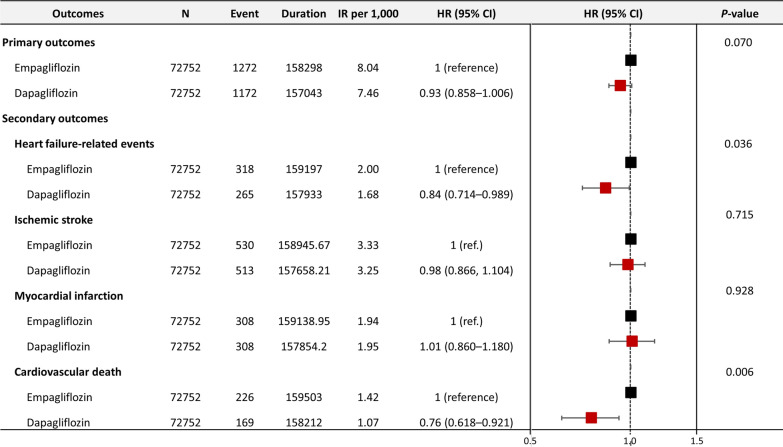
Methods: Korean National Health Insurance registry data between May 2016 and December 2018 were extracted, and an active-comparator new-user design was applied. The primary outcome was a composite of heart failure (HF)-related events (i.e., hospitalization for HF and HF-related death), myocardial infarction, ischemic stroke, and cardiovascular death. The secondary outcomes were individual components of the primary outcome.
Results: A total of 366,031 new users of dapagliflozin or empagliflozin were identified. After 1:1 nearest-neighbor propensity score matching, 72,752 individuals (mean age approximately 56 years, 42% women) from each group were included in the final analysis, with a follow-up of 150,000 ~ person-years. Approximately 40% of the patients included in the study had type 2 diabetes mellitus as their sole cardiovascular risk factor, with no other risk factors. The risk of the primary outcome was not different significantly between dapagliflozin and empagliflozin users (hazard ratio [HR] 0.93, 95% confidence interval [CI] 0.855-1.006). The risks of secondary outcomes were also similar, with the exception of the risks of HF-related events (HR 0.84, 95% CI 0.714-0.989) and cardiovascular death (HR 0.76, 95% CI 0.618-0.921), which were significantly lower in the dapagliflozin users.
Conclusions: This large-scale nationwide population-based real-world cohort study revealed no significant difference in composite cardiovascular outcomes between new users of dapagliflozin and empagliflozin. However, dapagliflozin might be associated with lower risks of hospitalization or death due to HF and cardiovascular death than empagliflozin in Asian patients with type 2 diabetes mellitus.
Keywords: Cardiovascular death; Cardiovascular risk; Dapagliflozin; Empagliflozin; Heart failure; Sodium-glucose co-transporter-2 inhibitors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Kosiborod M, Cavender MA, Fu AZ, Wilding JP, Khunti K, Holl RW, Norhammar A, Birkeland KI, Jørgensen ME, Thuresson M. Lower risk of heart failure and death in patients initiated on sodium-glucose cotransporter-2 inhibitors versus other glucose-lowering drugs: the CVD-REAL study (comparative effectiveness of cardiovascular outcomes in new users of sodium-glucose cotransporter-2 inhibitors) Circulation. 2017;136(3):249–59. doi: 10.1161/CIRCULATIONAHA.117.029190. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
