

Pediatric Maxillofacial Trauma: Insights into Diagnosis and Treatment of Mandibular Fractures in Pediatric Patients
- PMID: 37496941
- PMCID: PMC10367286
- DOI: 10.5005/jp-journals-10005-2401
Pediatric Maxillofacial Trauma: Insights into Diagnosis and Treatment of Mandibular Fractures in Pediatric Patients
Abstract
Aim: To assess the diagnostic and therapeutic approaches in pediatric mandibular fractures with regards to fracture pattern and localization.
Patients and methods: This retrospective study included patients under the age of 17 years that presented to the Department of Oral and Maxillofacial Surgery at Charité-Universitätsmedizin Berlin with mandibular fractures over an 11-year long period (2010-2020). Medical records were analyzed for age, gender, injury mechanism, clinical presentation, imaging modalities, fracture pattern, and fracture management. Statistical analyses included descriptive statistics, normality testing, and Mann-Whitney U tests.
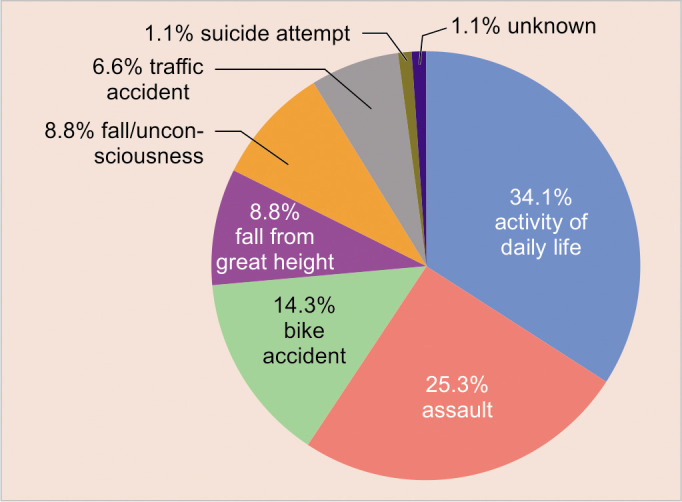
Results: A total of 91 pediatric patients (23 females and 68 males) presented with mandibular fractures. The majority of mandibular fractures occurred in patients aged 13-16 years (67.0%, n = 61). The main causes were activities of daily life (34.1%), followed by assault (25.3%). Malocclusion and pain upon mandibular joint compression were documented in 72.5% and 51.7% of patients, respectively. The most frequently applied radiological diagnostic tool was a panoramic X-ray (49.5%). The main fracture patterns were single (42.9%) and double fractures (48.4%). An age-adapted surgical approach using open reduction and internal fixation (ORIF) was the most frequent management (61.5%). A conservative approach was favored in cases of condylar head fractures. Resorbable plates were used in eight cases of ORIF (8.8%).
Conclusion: Treatment regimens should be carefully selected based on the unique anatomy of the pediatric patient with regards to centers of growth and dentition phase, to restore stomatognathic function and to maintain adequate skeletal growth and eruption of teeth.
Clinical significance: This study illustrates the challenges of mandibular fracture management in the pediatric patient.
How to cite this article: Hofmann E, Koerdt S, Heiland M, et al. Pediatric Maxillofacial Trauma: Insights into Diagnosis and Treatment of Mandibular Fractures in Pediatric Patients. Int J Clin Pediatr Dent 2023;16(3):499-509.
Keywords: Fracture management; Mandibular fracture; Pediatric maxillofacial trauma; Pediatric patient.
Copyright © 2023; The Author(s).
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures



References
-
- Rogan DT, Ahmed A. Pediatric facial fractures. Treasure Island (FL): StatPearls Publishing; 2021. [updated 2021 Jul 31]. Available at: - PubMed
Publication types
LinkOut - more resources
Full Text Sources